- UWF Libraries

Literature Review: Conducting & Writing
- Sample Literature Reviews
- Steps for Conducting a Lit Review
- Finding "The Literature"
- Organizing/Writing
- APA Style This link opens in a new window
- Chicago: Notes Bibliography This link opens in a new window
- MLA Style This link opens in a new window
Sample Lit Reviews from Communication Arts
Have an exemplary literature review.
- Literature Review Sample 1
- Literature Review Sample 2
- Literature Review Sample 3
Have you written a stellar literature review you care to share for teaching purposes?
Are you an instructor who has received an exemplary literature review and have permission from the student to post?
Please contact Britt McGowan at [email protected] for inclusion in this guide. All disciplines welcome and encouraged.
- << Previous: MLA Style
- Next: Get Help! >>
- Last Updated: Mar 22, 2024 9:37 AM
- URL: https://libguides.uwf.edu/litreview
Get science-backed answers as you write with Paperpal's Research feature
What is a Literature Review? How to Write It (with Examples)

A literature review is a critical analysis and synthesis of existing research on a particular topic. It provides an overview of the current state of knowledge, identifies gaps, and highlights key findings in the literature. 1 The purpose of a literature review is to situate your own research within the context of existing scholarship, demonstrating your understanding of the topic and showing how your work contributes to the ongoing conversation in the field. Learning how to write a literature review is a critical tool for successful research. Your ability to summarize and synthesize prior research pertaining to a certain topic demonstrates your grasp on the topic of study, and assists in the learning process.
Table of Contents
- What is the purpose of literature review?
- a. Habitat Loss and Species Extinction:
- b. Range Shifts and Phenological Changes:
- c. Ocean Acidification and Coral Reefs:
- d. Adaptive Strategies and Conservation Efforts:
- How to write a good literature review
- Choose a Topic and Define the Research Question:
- Decide on the Scope of Your Review:
- Select Databases for Searches:
- Conduct Searches and Keep Track:
- Review the Literature:
- Organize and Write Your Literature Review:
- Frequently asked questions
What is a literature review?
A well-conducted literature review demonstrates the researcher’s familiarity with the existing literature, establishes the context for their own research, and contributes to scholarly conversations on the topic. One of the purposes of a literature review is also to help researchers avoid duplicating previous work and ensure that their research is informed by and builds upon the existing body of knowledge.

What is the purpose of literature review?
A literature review serves several important purposes within academic and research contexts. Here are some key objectives and functions of a literature review: 2
- Contextualizing the Research Problem: The literature review provides a background and context for the research problem under investigation. It helps to situate the study within the existing body of knowledge.
- Identifying Gaps in Knowledge: By identifying gaps, contradictions, or areas requiring further research, the researcher can shape the research question and justify the significance of the study. This is crucial for ensuring that the new research contributes something novel to the field.
- Understanding Theoretical and Conceptual Frameworks: Literature reviews help researchers gain an understanding of the theoretical and conceptual frameworks used in previous studies. This aids in the development of a theoretical framework for the current research.
- Providing Methodological Insights: Another purpose of literature reviews is that it allows researchers to learn about the methodologies employed in previous studies. This can help in choosing appropriate research methods for the current study and avoiding pitfalls that others may have encountered.
- Establishing Credibility: A well-conducted literature review demonstrates the researcher’s familiarity with existing scholarship, establishing their credibility and expertise in the field. It also helps in building a solid foundation for the new research.
- Informing Hypotheses or Research Questions: The literature review guides the formulation of hypotheses or research questions by highlighting relevant findings and areas of uncertainty in existing literature.
Literature review example
Let’s delve deeper with a literature review example: Let’s say your literature review is about the impact of climate change on biodiversity. You might format your literature review into sections such as the effects of climate change on habitat loss and species extinction, phenological changes, and marine biodiversity. Each section would then summarize and analyze relevant studies in those areas, highlighting key findings and identifying gaps in the research. The review would conclude by emphasizing the need for further research on specific aspects of the relationship between climate change and biodiversity. The following literature review template provides a glimpse into the recommended literature review structure and content, demonstrating how research findings are organized around specific themes within a broader topic.
Literature Review on Climate Change Impacts on Biodiversity:
Climate change is a global phenomenon with far-reaching consequences, including significant impacts on biodiversity. This literature review synthesizes key findings from various studies:
a. Habitat Loss and Species Extinction:
Climate change-induced alterations in temperature and precipitation patterns contribute to habitat loss, affecting numerous species (Thomas et al., 2004). The review discusses how these changes increase the risk of extinction, particularly for species with specific habitat requirements.
b. Range Shifts and Phenological Changes:
Observations of range shifts and changes in the timing of biological events (phenology) are documented in response to changing climatic conditions (Parmesan & Yohe, 2003). These shifts affect ecosystems and may lead to mismatches between species and their resources.
c. Ocean Acidification and Coral Reefs:
The review explores the impact of climate change on marine biodiversity, emphasizing ocean acidification’s threat to coral reefs (Hoegh-Guldberg et al., 2007). Changes in pH levels negatively affect coral calcification, disrupting the delicate balance of marine ecosystems.
d. Adaptive Strategies and Conservation Efforts:
Recognizing the urgency of the situation, the literature review discusses various adaptive strategies adopted by species and conservation efforts aimed at mitigating the impacts of climate change on biodiversity (Hannah et al., 2007). It emphasizes the importance of interdisciplinary approaches for effective conservation planning.
How to write a good literature review
Writing a literature review involves summarizing and synthesizing existing research on a particular topic. A good literature review format should include the following elements.
Introduction: The introduction sets the stage for your literature review, providing context and introducing the main focus of your review.
- Opening Statement: Begin with a general statement about the broader topic and its significance in the field.
- Scope and Purpose: Clearly define the scope of your literature review. Explain the specific research question or objective you aim to address.
- Organizational Framework: Briefly outline the structure of your literature review, indicating how you will categorize and discuss the existing research.
- Significance of the Study: Highlight why your literature review is important and how it contributes to the understanding of the chosen topic.
- Thesis Statement: Conclude the introduction with a concise thesis statement that outlines the main argument or perspective you will develop in the body of the literature review.
Body: The body of the literature review is where you provide a comprehensive analysis of existing literature, grouping studies based on themes, methodologies, or other relevant criteria.
- Organize by Theme or Concept: Group studies that share common themes, concepts, or methodologies. Discuss each theme or concept in detail, summarizing key findings and identifying gaps or areas of disagreement.
- Critical Analysis: Evaluate the strengths and weaknesses of each study. Discuss the methodologies used, the quality of evidence, and the overall contribution of each work to the understanding of the topic.
- Synthesis of Findings: Synthesize the information from different studies to highlight trends, patterns, or areas of consensus in the literature.
- Identification of Gaps: Discuss any gaps or limitations in the existing research and explain how your review contributes to filling these gaps.
- Transition between Sections: Provide smooth transitions between different themes or concepts to maintain the flow of your literature review.
Conclusion: The conclusion of your literature review should summarize the main findings, highlight the contributions of the review, and suggest avenues for future research.
- Summary of Key Findings: Recap the main findings from the literature and restate how they contribute to your research question or objective.
- Contributions to the Field: Discuss the overall contribution of your literature review to the existing knowledge in the field.
- Implications and Applications: Explore the practical implications of the findings and suggest how they might impact future research or practice.
- Recommendations for Future Research: Identify areas that require further investigation and propose potential directions for future research in the field.
- Final Thoughts: Conclude with a final reflection on the importance of your literature review and its relevance to the broader academic community.

Conducting a literature review
Conducting a literature review is an essential step in research that involves reviewing and analyzing existing literature on a specific topic. It’s important to know how to do a literature review effectively, so here are the steps to follow: 1
Choose a Topic and Define the Research Question:
- Select a topic that is relevant to your field of study.
- Clearly define your research question or objective. Determine what specific aspect of the topic do you want to explore?
Decide on the Scope of Your Review:
- Determine the timeframe for your literature review. Are you focusing on recent developments, or do you want a historical overview?
- Consider the geographical scope. Is your review global, or are you focusing on a specific region?
- Define the inclusion and exclusion criteria. What types of sources will you include? Are there specific types of studies or publications you will exclude?
Select Databases for Searches:
- Identify relevant databases for your field. Examples include PubMed, IEEE Xplore, Scopus, Web of Science, and Google Scholar.
- Consider searching in library catalogs, institutional repositories, and specialized databases related to your topic.
Conduct Searches and Keep Track:
- Develop a systematic search strategy using keywords, Boolean operators (AND, OR, NOT), and other search techniques.
- Record and document your search strategy for transparency and replicability.
- Keep track of the articles, including publication details, abstracts, and links. Use citation management tools like EndNote, Zotero, or Mendeley to organize your references.
Review the Literature:
- Evaluate the relevance and quality of each source. Consider the methodology, sample size, and results of studies.
- Organize the literature by themes or key concepts. Identify patterns, trends, and gaps in the existing research.
- Summarize key findings and arguments from each source. Compare and contrast different perspectives.
- Identify areas where there is a consensus in the literature and where there are conflicting opinions.
- Provide critical analysis and synthesis of the literature. What are the strengths and weaknesses of existing research?
Organize and Write Your Literature Review:
- Literature review outline should be based on themes, chronological order, or methodological approaches.
- Write a clear and coherent narrative that synthesizes the information gathered.
- Use proper citations for each source and ensure consistency in your citation style (APA, MLA, Chicago, etc.).
- Conclude your literature review by summarizing key findings, identifying gaps, and suggesting areas for future research.
The literature review sample and detailed advice on writing and conducting a review will help you produce a well-structured report. But remember that a literature review is an ongoing process, and it may be necessary to revisit and update it as your research progresses.
Frequently asked questions
A literature review is a critical and comprehensive analysis of existing literature (published and unpublished works) on a specific topic or research question and provides a synthesis of the current state of knowledge in a particular field. A well-conducted literature review is crucial for researchers to build upon existing knowledge, avoid duplication of efforts, and contribute to the advancement of their field. It also helps researchers situate their work within a broader context and facilitates the development of a sound theoretical and conceptual framework for their studies.
Literature review is a crucial component of research writing, providing a solid background for a research paper’s investigation. The aim is to keep professionals up to date by providing an understanding of ongoing developments within a specific field, including research methods, and experimental techniques used in that field, and present that knowledge in the form of a written report. Also, the depth and breadth of the literature review emphasizes the credibility of the scholar in his or her field.
Before writing a literature review, it’s essential to undertake several preparatory steps to ensure that your review is well-researched, organized, and focused. This includes choosing a topic of general interest to you and doing exploratory research on that topic, writing an annotated bibliography, and noting major points, especially those that relate to the position you have taken on the topic.
Literature reviews and academic research papers are essential components of scholarly work but serve different purposes within the academic realm. 3 A literature review aims to provide a foundation for understanding the current state of research on a particular topic, identify gaps or controversies, and lay the groundwork for future research. Therefore, it draws heavily from existing academic sources, including books, journal articles, and other scholarly publications. In contrast, an academic research paper aims to present new knowledge, contribute to the academic discourse, and advance the understanding of a specific research question. Therefore, it involves a mix of existing literature (in the introduction and literature review sections) and original data or findings obtained through research methods.
Literature reviews are essential components of academic and research papers, and various strategies can be employed to conduct them effectively. If you want to know how to write a literature review for a research paper, here are four common approaches that are often used by researchers. Chronological Review: This strategy involves organizing the literature based on the chronological order of publication. It helps to trace the development of a topic over time, showing how ideas, theories, and research have evolved. Thematic Review: Thematic reviews focus on identifying and analyzing themes or topics that cut across different studies. Instead of organizing the literature chronologically, it is grouped by key themes or concepts, allowing for a comprehensive exploration of various aspects of the topic. Methodological Review: This strategy involves organizing the literature based on the research methods employed in different studies. It helps to highlight the strengths and weaknesses of various methodologies and allows the reader to evaluate the reliability and validity of the research findings. Theoretical Review: A theoretical review examines the literature based on the theoretical frameworks used in different studies. This approach helps to identify the key theories that have been applied to the topic and assess their contributions to the understanding of the subject. It’s important to note that these strategies are not mutually exclusive, and a literature review may combine elements of more than one approach. The choice of strategy depends on the research question, the nature of the literature available, and the goals of the review. Additionally, other strategies, such as integrative reviews or systematic reviews, may be employed depending on the specific requirements of the research.
The literature review format can vary depending on the specific publication guidelines. However, there are some common elements and structures that are often followed. Here is a general guideline for the format of a literature review: Introduction: Provide an overview of the topic. Define the scope and purpose of the literature review. State the research question or objective. Body: Organize the literature by themes, concepts, or chronology. Critically analyze and evaluate each source. Discuss the strengths and weaknesses of the studies. Highlight any methodological limitations or biases. Identify patterns, connections, or contradictions in the existing research. Conclusion: Summarize the key points discussed in the literature review. Highlight the research gap. Address the research question or objective stated in the introduction. Highlight the contributions of the review and suggest directions for future research.
Both annotated bibliographies and literature reviews involve the examination of scholarly sources. While annotated bibliographies focus on individual sources with brief annotations, literature reviews provide a more in-depth, integrated, and comprehensive analysis of existing literature on a specific topic. The key differences are as follows:
References
- Denney, A. S., & Tewksbury, R. (2013). How to write a literature review. Journal of criminal justice education , 24 (2), 218-234.
- Pan, M. L. (2016). Preparing literature reviews: Qualitative and quantitative approaches . Taylor & Francis.
- Cantero, C. (2019). How to write a literature review. San José State University Writing Center .
Paperpal is an AI writing assistant that help academics write better, faster with real-time suggestions for in-depth language and grammar correction. Trained on millions of research manuscripts enhanced by professional academic editors, Paperpal delivers human precision at machine speed.
Try it for free or upgrade to Paperpal Prime , which unlocks unlimited access to premium features like academic translation, paraphrasing, contextual synonyms, consistency checks and more. It’s like always having a professional academic editor by your side! Go beyond limitations and experience the future of academic writing. Get Paperpal Prime now at just US$19 a month!
Related Reads:
- Empirical Research: A Comprehensive Guide for Academics
- How to Write a Scientific Paper in 10 Steps
- Life Sciences Papers: 9 Tips for Authors Writing in Biological Sciences
- What is an Argumentative Essay? How to Write It (With Examples)
6 Tips for Post-Doc Researchers to Take Their Career to the Next Level
Self-plagiarism in research: what it is and how to avoid it, you may also like, 4 ways paperpal encourages responsible writing with ai, what are scholarly sources and where can you..., how to write a hypothesis types and examples , measuring academic success: definition & strategies for excellence, what is academic writing: tips for students, why traditional editorial process needs an upgrade, paperpal’s new ai research finder empowers authors to..., what is hedging in academic writing , how to use ai to enhance your college..., ai + human expertise – a paradigm shift....
Purdue Online Writing Lab Purdue OWL® College of Liberal Arts
Writing a Literature Review

Welcome to the Purdue OWL
This page is brought to you by the OWL at Purdue University. When printing this page, you must include the entire legal notice.
Copyright ©1995-2018 by The Writing Lab & The OWL at Purdue and Purdue University. All rights reserved. This material may not be published, reproduced, broadcast, rewritten, or redistributed without permission. Use of this site constitutes acceptance of our terms and conditions of fair use.
A literature review is a document or section of a document that collects key sources on a topic and discusses those sources in conversation with each other (also called synthesis ). The lit review is an important genre in many disciplines, not just literature (i.e., the study of works of literature such as novels and plays). When we say “literature review” or refer to “the literature,” we are talking about the research ( scholarship ) in a given field. You will often see the terms “the research,” “the scholarship,” and “the literature” used mostly interchangeably.
Where, when, and why would I write a lit review?
There are a number of different situations where you might write a literature review, each with slightly different expectations; different disciplines, too, have field-specific expectations for what a literature review is and does. For instance, in the humanities, authors might include more overt argumentation and interpretation of source material in their literature reviews, whereas in the sciences, authors are more likely to report study designs and results in their literature reviews; these differences reflect these disciplines’ purposes and conventions in scholarship. You should always look at examples from your own discipline and talk to professors or mentors in your field to be sure you understand your discipline’s conventions, for literature reviews as well as for any other genre.
A literature review can be a part of a research paper or scholarly article, usually falling after the introduction and before the research methods sections. In these cases, the lit review just needs to cover scholarship that is important to the issue you are writing about; sometimes it will also cover key sources that informed your research methodology.
Lit reviews can also be standalone pieces, either as assignments in a class or as publications. In a class, a lit review may be assigned to help students familiarize themselves with a topic and with scholarship in their field, get an idea of the other researchers working on the topic they’re interested in, find gaps in existing research in order to propose new projects, and/or develop a theoretical framework and methodology for later research. As a publication, a lit review usually is meant to help make other scholars’ lives easier by collecting and summarizing, synthesizing, and analyzing existing research on a topic. This can be especially helpful for students or scholars getting into a new research area, or for directing an entire community of scholars toward questions that have not yet been answered.
What are the parts of a lit review?
Most lit reviews use a basic introduction-body-conclusion structure; if your lit review is part of a larger paper, the introduction and conclusion pieces may be just a few sentences while you focus most of your attention on the body. If your lit review is a standalone piece, the introduction and conclusion take up more space and give you a place to discuss your goals, research methods, and conclusions separately from where you discuss the literature itself.
Introduction:
- An introductory paragraph that explains what your working topic and thesis is
- A forecast of key topics or texts that will appear in the review
- Potentially, a description of how you found sources and how you analyzed them for inclusion and discussion in the review (more often found in published, standalone literature reviews than in lit review sections in an article or research paper)
- Summarize and synthesize: Give an overview of the main points of each source and combine them into a coherent whole
- Analyze and interpret: Don’t just paraphrase other researchers – add your own interpretations where possible, discussing the significance of findings in relation to the literature as a whole
- Critically Evaluate: Mention the strengths and weaknesses of your sources
- Write in well-structured paragraphs: Use transition words and topic sentence to draw connections, comparisons, and contrasts.
Conclusion:
- Summarize the key findings you have taken from the literature and emphasize their significance
- Connect it back to your primary research question
How should I organize my lit review?
Lit reviews can take many different organizational patterns depending on what you are trying to accomplish with the review. Here are some examples:
- Chronological : The simplest approach is to trace the development of the topic over time, which helps familiarize the audience with the topic (for instance if you are introducing something that is not commonly known in your field). If you choose this strategy, be careful to avoid simply listing and summarizing sources in order. Try to analyze the patterns, turning points, and key debates that have shaped the direction of the field. Give your interpretation of how and why certain developments occurred (as mentioned previously, this may not be appropriate in your discipline — check with a teacher or mentor if you’re unsure).
- Thematic : If you have found some recurring central themes that you will continue working with throughout your piece, you can organize your literature review into subsections that address different aspects of the topic. For example, if you are reviewing literature about women and religion, key themes can include the role of women in churches and the religious attitude towards women.
- Qualitative versus quantitative research
- Empirical versus theoretical scholarship
- Divide the research by sociological, historical, or cultural sources
- Theoretical : In many humanities articles, the literature review is the foundation for the theoretical framework. You can use it to discuss various theories, models, and definitions of key concepts. You can argue for the relevance of a specific theoretical approach or combine various theorical concepts to create a framework for your research.
What are some strategies or tips I can use while writing my lit review?
Any lit review is only as good as the research it discusses; make sure your sources are well-chosen and your research is thorough. Don’t be afraid to do more research if you discover a new thread as you’re writing. More info on the research process is available in our "Conducting Research" resources .
As you’re doing your research, create an annotated bibliography ( see our page on the this type of document ). Much of the information used in an annotated bibliography can be used also in a literature review, so you’ll be not only partially drafting your lit review as you research, but also developing your sense of the larger conversation going on among scholars, professionals, and any other stakeholders in your topic.
Usually you will need to synthesize research rather than just summarizing it. This means drawing connections between sources to create a picture of the scholarly conversation on a topic over time. Many student writers struggle to synthesize because they feel they don’t have anything to add to the scholars they are citing; here are some strategies to help you:
- It often helps to remember that the point of these kinds of syntheses is to show your readers how you understand your research, to help them read the rest of your paper.
- Writing teachers often say synthesis is like hosting a dinner party: imagine all your sources are together in a room, discussing your topic. What are they saying to each other?
- Look at the in-text citations in each paragraph. Are you citing just one source for each paragraph? This usually indicates summary only. When you have multiple sources cited in a paragraph, you are more likely to be synthesizing them (not always, but often
- Read more about synthesis here.
The most interesting literature reviews are often written as arguments (again, as mentioned at the beginning of the page, this is discipline-specific and doesn’t work for all situations). Often, the literature review is where you can establish your research as filling a particular gap or as relevant in a particular way. You have some chance to do this in your introduction in an article, but the literature review section gives a more extended opportunity to establish the conversation in the way you would like your readers to see it. You can choose the intellectual lineage you would like to be part of and whose definitions matter most to your thinking (mostly humanities-specific, but this goes for sciences as well). In addressing these points, you argue for your place in the conversation, which tends to make the lit review more compelling than a simple reporting of other sources.

Literature Review Guide: Examples of Literature Reviews
- What is a Literature Review?
- How to start?
- Search strategies and Databases
- Examples of Literature Reviews
- How to organise the review
- Library summary
- Emerald Infographic
All good quality journal articles will include a small Literature Review after the Introduction paragraph. It may not be called a Literature Review but gives you an idea of how one is created in miniature.
Sample Literature Reviews as part of a articles or Theses
- Sample Literature Review on Critical Thinking (Gwendolyn Reece, American University Library)
- Hackett, G and Melia, D . The hotel as the holiday/stay destination:trends and innovations. Presented at TRIC Conference, Belfast, Ireland- June 2012 and EuroCHRIE Conference
Links to sample Literature Reviews from other libraries
- Sample literature reviews from University of West Florida
Standalone Literature Reviews
- Attitudes towards the Disability in Ireland
- Martin, A., O'Connor-Fenelon, M. and Lyons, R. (2010). Non-verbal communication between nurses and people with an intellectual disability: A review of the literature. Journal of Intellectual Diabilities, 14(4), 303-314.
Irish Theses
- Phillips, Martin (2015) European airline performance: a data envelopment analysis with extrapolations based on model outputs. Master of Business Studies thesis, Dublin City University.
- The customers’ perception of servicescape’s influence on their behaviours, in the food retail industry : Dublin Business School 2015
- Coughlan, Ray (2015) What was the role of leadership in the transformation of a failing Irish Insurance business. Masters thesis, Dublin, National College of Ireland.
- << Previous: Search strategies and Databases
- Next: Tutorials >>
- Last Updated: Feb 27, 2024 4:07 PM
- URL: https://ait.libguides.com/literaturereview
- Resources Home 🏠
- Try SciSpace Copilot
- Search research papers
- Add Copilot Extension
- Try AI Detector
- Try Paraphraser
- Try Citation Generator
- April Papers
- June Papers
- July Papers

How To Write A Literature Review - A Complete Guide

Table of Contents
A literature review is much more than just another section in your research paper. It forms the very foundation of your research. It is a formal piece of writing where you analyze the existing theoretical framework, principles, and assumptions and use that as a base to shape your approach to the research question.
Curating and drafting a solid literature review section not only lends more credibility to your research paper but also makes your research tighter and better focused. But, writing literature reviews is a difficult task. It requires extensive reading, plus you have to consider market trends and technological and political changes, which tend to change in the blink of an eye.
Now streamline your literature review process with the help of SciSpace Copilot. With this AI research assistant, you can efficiently synthesize and analyze a vast amount of information, identify key themes and trends, and uncover gaps in the existing research. Get real-time explanations, summaries, and answers to your questions for the paper you're reviewing, making navigating and understanding the complex literature landscape easier.

In this comprehensive guide, we will explore everything from the definition of a literature review, its appropriate length, various types of literature reviews, and how to write one.
What is a literature review?
A literature review is a collation of survey, research, critical evaluation, and assessment of the existing literature in a preferred domain.
Eminent researcher and academic Arlene Fink, in her book Conducting Research Literature Reviews , defines it as the following:
“A literature review surveys books, scholarly articles, and any other sources relevant to a particular issue, area of research, or theory, and by so doing, provides a description, summary, and critical evaluation of these works in relation to the research problem being investigated.
Literature reviews are designed to provide an overview of sources you have explored while researching a particular topic, and to demonstrate to your readers how your research fits within a larger field of study.”
Simply put, a literature review can be defined as a critical discussion of relevant pre-existing research around your research question and carving out a definitive place for your study in the existing body of knowledge. Literature reviews can be presented in multiple ways: a section of an article, the whole research paper itself, or a chapter of your thesis.

A literature review does function as a summary of sources, but it also allows you to analyze further, interpret, and examine the stated theories, methods, viewpoints, and, of course, the gaps in the existing content.
As an author, you can discuss and interpret the research question and its various aspects and debate your adopted methods to support the claim.
What is the purpose of a literature review?
A literature review is meant to help your readers understand the relevance of your research question and where it fits within the existing body of knowledge. As a researcher, you should use it to set the context, build your argument, and establish the need for your study.
What is the importance of a literature review?
The literature review is a critical part of research papers because it helps you:
- Gain an in-depth understanding of your research question and the surrounding area
- Convey that you have a thorough understanding of your research area and are up-to-date with the latest changes and advancements
- Establish how your research is connected or builds on the existing body of knowledge and how it could contribute to further research
- Elaborate on the validity and suitability of your theoretical framework and research methodology
- Identify and highlight gaps and shortcomings in the existing body of knowledge and how things need to change
- Convey to readers how your study is different or how it contributes to the research area
How long should a literature review be?
Ideally, the literature review should take up 15%-40% of the total length of your manuscript. So, if you have a 10,000-word research paper, the minimum word count could be 1500.
Your literature review format depends heavily on the kind of manuscript you are writing — an entire chapter in case of doctoral theses, a part of the introductory section in a research article, to a full-fledged review article that examines the previously published research on a topic.
Another determining factor is the type of research you are doing. The literature review section tends to be longer for secondary research projects than primary research projects.
What are the different types of literature reviews?
All literature reviews are not the same. There are a variety of possible approaches that you can take. It all depends on the type of research you are pursuing.
Here are the different types of literature reviews:
Argumentative review
It is called an argumentative review when you carefully present literature that only supports or counters a specific argument or premise to establish a viewpoint.
Integrative review
It is a type of literature review focused on building a comprehensive understanding of a topic by combining available theoretical frameworks and empirical evidence.
Methodological review
This approach delves into the ''how'' and the ''what" of the research question — you cannot look at the outcome in isolation; you should also review the methodology used.
Systematic review
This form consists of an overview of existing evidence pertinent to a clearly formulated research question, which uses pre-specified and standardized methods to identify and critically appraise relevant research and collect, report, and analyze data from the studies included in the review.
Meta-analysis review
Meta-analysis uses statistical methods to summarize the results of independent studies. By combining information from all relevant studies, meta-analysis can provide more precise estimates of the effects than those derived from the individual studies included within a review.
Historical review
Historical literature reviews focus on examining research throughout a period, often starting with the first time an issue, concept, theory, or phenomenon emerged in the literature, then tracing its evolution within the scholarship of a discipline. The purpose is to place research in a historical context to show familiarity with state-of-the-art developments and identify future research's likely directions.
Theoretical Review
This form aims to examine the corpus of theory accumulated regarding an issue, concept, theory, and phenomenon. The theoretical literature review helps to establish what theories exist, the relationships between them, the degree the existing approaches have been investigated, and to develop new hypotheses to be tested.
Scoping Review
The Scoping Review is often used at the beginning of an article, dissertation, or research proposal. It is conducted before the research to highlight gaps in the existing body of knowledge and explains why the project should be greenlit.
State-of-the-Art Review
The State-of-the-Art review is conducted periodically, focusing on the most recent research. It describes what is currently known, understood, or agreed upon regarding the research topic and highlights where there are still disagreements.
Can you use the first person in a literature review?
When writing literature reviews, you should avoid the usage of first-person pronouns. It means that instead of "I argue that" or "we argue that," the appropriate expression would be "this research paper argues that."
Do you need an abstract for a literature review?
Ideally, yes. It is always good to have a condensed summary that is self-contained and independent of the rest of your review. As for how to draft one, you can follow the same fundamental idea when preparing an abstract for a literature review. It should also include:
- The research topic and your motivation behind selecting it
- A one-sentence thesis statement
- An explanation of the kinds of literature featured in the review
- Summary of what you've learned
- Conclusions you drew from the literature you reviewed
- Potential implications and future scope for research
Here's an example of the abstract of a literature review

Is a literature review written in the past tense?
Yes, the literature review should ideally be written in the past tense. You should not use the present or future tense when writing one. The exceptions are when you have statements describing events that happened earlier than the literature you are reviewing or events that are currently occurring; then, you can use the past perfect or present perfect tenses.
How many sources for a literature review?
There are multiple approaches to deciding how many sources to include in a literature review section. The first approach would be to look level you are at as a researcher. For instance, a doctoral thesis might need 60+ sources. In contrast, you might only need to refer to 5-15 sources at the undergraduate level.
The second approach is based on the kind of literature review you are doing — whether it is merely a chapter of your paper or if it is a self-contained paper in itself. When it is just a chapter, sources should equal the total number of pages in your article's body. In the second scenario, you need at least three times as many sources as there are pages in your work.
Quick tips on how to write a literature review
To know how to write a literature review, you must clearly understand its impact and role in establishing your work as substantive research material.
You need to follow the below-mentioned steps, to write a literature review:
- Outline the purpose behind the literature review
- Search relevant literature
- Examine and assess the relevant resources
- Discover connections by drawing deep insights from the resources
- Structure planning to write a good literature review
1. Outline and identify the purpose of a literature review
As a first step on how to write a literature review, you must know what the research question or topic is and what shape you want your literature review to take. Ensure you understand the research topic inside out, or else seek clarifications. You must be able to the answer below questions before you start:
- How many sources do I need to include?
- What kind of sources should I analyze?
- How much should I critically evaluate each source?
- Should I summarize, synthesize or offer a critique of the sources?
- Do I need to include any background information or definitions?
Additionally, you should know that the narrower your research topic is, the swifter it will be for you to restrict the number of sources to be analyzed.
2. Search relevant literature
Dig deeper into search engines to discover what has already been published around your chosen topic. Make sure you thoroughly go through appropriate reference sources like books, reports, journal articles, government docs, and web-based resources.
You must prepare a list of keywords and their different variations. You can start your search from any library’s catalog, provided you are an active member of that institution. The exact keywords can be extended to widen your research over other databases and academic search engines like:
- Google Scholar
- Microsoft Academic
- Science.gov
Besides, it is not advisable to go through every resource word by word. Alternatively, what you can do is you can start by reading the abstract and then decide whether that source is relevant to your research or not.
Additionally, you must spend surplus time assessing the quality and relevance of resources. It would help if you tried preparing a list of citations to ensure that there lies no repetition of authors, publications, or articles in the literature review.
3. Examine and assess the sources
It is nearly impossible for you to go through every detail in the research article. So rather than trying to fetch every detail, you have to analyze and decide which research sources resemble closest and appear relevant to your chosen domain.
While analyzing the sources, you should look to find out answers to questions like:
- What question or problem has the author been describing and debating?
- What is the definition of critical aspects?
- How well the theories, approach, and methodology have been explained?
- Whether the research theory used some conventional or new innovative approach?
- How relevant are the key findings of the work?
- In what ways does it relate to other sources on the same topic?
- What challenges does this research paper pose to the existing theory
- What are the possible contributions or benefits it adds to the subject domain?
Be always mindful that you refer only to credible and authentic resources. It would be best if you always take references from different publications to validate your theory.
Always keep track of important information or data you can present in your literature review right from the beginning. It will help steer your path from any threats of plagiarism and also make it easier to curate an annotated bibliography or reference section.
4. Discover connections
At this stage, you must start deciding on the argument and structure of your literature review. To accomplish this, you must discover and identify the relations and connections between various resources while drafting your abstract.
A few aspects that you should be aware of while writing a literature review include:
- Rise to prominence: Theories and methods that have gained reputation and supporters over time.
- Constant scrutiny: Concepts or theories that repeatedly went under examination.
- Contradictions and conflicts: Theories, both the supporting and the contradictory ones, for the research topic.
- Knowledge gaps: What exactly does it fail to address, and how to bridge them with further research?
- Influential resources: Significant research projects available that have been upheld as milestones or perhaps, something that can modify the current trends
Once you join the dots between various past research works, it will be easier for you to draw a conclusion and identify your contribution to the existing knowledge base.
5. Structure planning to write a good literature review
There exist different ways towards planning and executing the structure of a literature review. The format of a literature review varies and depends upon the length of the research.
Like any other research paper, the literature review format must contain three sections: introduction, body, and conclusion. The goals and objectives of the research question determine what goes inside these three sections.
Nevertheless, a good literature review can be structured according to the chronological, thematic, methodological, or theoretical framework approach.
Literature review samples
1. Standalone

2. As a section of a research paper

How SciSpace Discover makes literature review a breeze?
SciSpace Discover is a one-stop solution to do an effective literature search and get barrier-free access to scientific knowledge. It is an excellent repository where you can find millions of only peer-reviewed articles and full-text PDF files. Here’s more on how you can use it:
Find the right information

Find what you want quickly and easily with comprehensive search filters that let you narrow down papers according to PDF availability, year of publishing, document type, and affiliated institution. Moreover, you can sort the results based on the publishing date, citation count, and relevance.
Assess credibility of papers quickly

When doing the literature review, it is critical to establish the quality of your sources. They form the foundation of your research. SciSpace Discover helps you assess the quality of a source by providing an overview of its references, citations, and performance metrics.
Get the complete picture in no time

SciSpace Discover’s personalized suggestion engine helps you stay on course and get the complete picture of the topic from one place. Every time you visit an article page, it provides you links to related papers. Besides that, it helps you understand what’s trending, who are the top authors, and who are the leading publishers on a topic.
Make referring sources super easy

To ensure you don't lose track of your sources, you must start noting down your references when doing the literature review. SciSpace Discover makes this step effortless. Click the 'cite' button on an article page, and you will receive preloaded citation text in multiple styles — all you've to do is copy-paste it into your manuscript.
Final tips on how to write a literature review
A massive chunk of time and effort is required to write a good literature review. But, if you go about it systematically, you'll be able to save a ton of time and build a solid foundation for your research.
We hope this guide has helped you answer several key questions you have about writing literature reviews.
Would you like to explore SciSpace Discover and kick off your literature search right away? You can get started here .
Frequently Asked Questions (FAQs)
1. how to start a literature review.
• What questions do you want to answer?
• What sources do you need to answer these questions?
• What information do these sources contain?
• How can you use this information to answer your questions?
2. What to include in a literature review?
• A brief background of the problem or issue
• What has previously been done to address the problem or issue
• A description of what you will do in your project
• How this study will contribute to research on the subject
3. Why literature review is important?
The literature review is an important part of any research project because it allows the writer to look at previous studies on a topic and determine existing gaps in the literature, as well as what has already been done. It will also help them to choose the most appropriate method for their own study.
4. How to cite a literature review in APA format?
To cite a literature review in APA style, you need to provide the author's name, the title of the article, and the year of publication. For example: Patel, A. B., & Stokes, G. S. (2012). The relationship between personality and intelligence: A meta-analysis of longitudinal research. Personality and Individual Differences, 53(1), 16-21
5. What are the components of a literature review?
• A brief introduction to the topic, including its background and context. The introduction should also include a rationale for why the study is being conducted and what it will accomplish.
• A description of the methodologies used in the study. This can include information about data collection methods, sample size, and statistical analyses.
• A presentation of the findings in an organized format that helps readers follow along with the author's conclusions.
6. What are common errors in writing literature review?
• Not spending enough time to critically evaluate the relevance of resources, observations and conclusions.
• Totally relying on secondary data while ignoring primary data.
• Letting your personal bias seep into your interpretation of existing literature.
• No detailed explanation of the procedure to discover and identify an appropriate literature review.
7. What are the 5 C's of writing literature review?
• Cite - the sources you utilized and referenced in your research.
• Compare - existing arguments, hypotheses, methodologies, and conclusions found in the knowledge base.
• Contrast - the arguments, topics, methodologies, approaches, and disputes that may be found in the literature.
• Critique - the literature and describe the ideas and opinions you find more convincing and why.
• Connect - the various studies you reviewed in your research.
8. How many sources should a literature review have?
When it is just a chapter, sources should equal the total number of pages in your article's body. if it is a self-contained paper in itself, you need at least three times as many sources as there are pages in your work.
9. Can literature review have diagrams?
• To represent an abstract idea or concept
• To explain the steps of a process or procedure
• To help readers understand the relationships between different concepts
10. How old should sources be in a literature review?
Sources for a literature review should be as current as possible or not older than ten years. The only exception to this rule is if you are reviewing a historical topic and need to use older sources.
11. What are the types of literature review?
• Argumentative review
• Integrative review
• Methodological review
• Systematic review
• Meta-analysis review
• Historical review
• Theoretical review
• Scoping review
• State-of-the-Art review
12. Is a literature review mandatory?
Yes. Literature review is a mandatory part of any research project. It is a critical step in the process that allows you to establish the scope of your research, and provide a background for the rest of your work.
But before you go,
- Six Online Tools for Easy Literature Review
- Evaluating literature review: systematic vs. scoping reviews
- Systematic Approaches to a Successful Literature Review
- Writing Integrative Literature Reviews: Guidelines and Examples
You might also like

Consensus GPT vs. SciSpace GPT: Choose the Best GPT for Research

Literature Review and Theoretical Framework: Understanding the Differences

Types of Essays in Academic Writing - Quick Guide (2024)
Have a language expert improve your writing
Run a free plagiarism check in 10 minutes, automatically generate references for free.
- Knowledge Base
- Dissertation
- What is a Literature Review? | Guide, Template, & Examples
What is a Literature Review? | Guide, Template, & Examples
Published on 22 February 2022 by Shona McCombes . Revised on 7 June 2022.
What is a literature review? A literature review is a survey of scholarly sources on a specific topic. It provides an overview of current knowledge, allowing you to identify relevant theories, methods, and gaps in the existing research.
There are five key steps to writing a literature review:
- Search for relevant literature
- Evaluate sources
- Identify themes, debates and gaps
- Outline the structure
- Write your literature review
A good literature review doesn’t just summarise sources – it analyses, synthesises, and critically evaluates to give a clear picture of the state of knowledge on the subject.
Instantly correct all language mistakes in your text
Be assured that you'll submit flawless writing. Upload your document to correct all your mistakes.

Table of contents
Why write a literature review, examples of literature reviews, step 1: search for relevant literature, step 2: evaluate and select sources, step 3: identify themes, debates and gaps, step 4: outline your literature review’s structure, step 5: write your literature review, frequently asked questions about literature reviews, introduction.
- Quick Run-through
- Step 1 & 2
When you write a dissertation or thesis, you will have to conduct a literature review to situate your research within existing knowledge. The literature review gives you a chance to:
- Demonstrate your familiarity with the topic and scholarly context
- Develop a theoretical framework and methodology for your research
- Position yourself in relation to other researchers and theorists
- Show how your dissertation addresses a gap or contributes to a debate
You might also have to write a literature review as a stand-alone assignment. In this case, the purpose is to evaluate the current state of research and demonstrate your knowledge of scholarly debates around a topic.
The content will look slightly different in each case, but the process of conducting a literature review follows the same steps. We’ve written a step-by-step guide that you can follow below.

The only proofreading tool specialized in correcting academic writing
The academic proofreading tool has been trained on 1000s of academic texts and by native English editors. Making it the most accurate and reliable proofreading tool for students.

Correct my document today
Writing literature reviews can be quite challenging! A good starting point could be to look at some examples, depending on what kind of literature review you’d like to write.
- Example literature review #1: “Why Do People Migrate? A Review of the Theoretical Literature” ( Theoretical literature review about the development of economic migration theory from the 1950s to today.)
- Example literature review #2: “Literature review as a research methodology: An overview and guidelines” ( Methodological literature review about interdisciplinary knowledge acquisition and production.)
- Example literature review #3: “The Use of Technology in English Language Learning: A Literature Review” ( Thematic literature review about the effects of technology on language acquisition.)
- Example literature review #4: “Learners’ Listening Comprehension Difficulties in English Language Learning: A Literature Review” ( Chronological literature review about how the concept of listening skills has changed over time.)
You can also check out our templates with literature review examples and sample outlines at the links below.
Download Word doc Download Google doc
Before you begin searching for literature, you need a clearly defined topic .
If you are writing the literature review section of a dissertation or research paper, you will search for literature related to your research objectives and questions .
If you are writing a literature review as a stand-alone assignment, you will have to choose a focus and develop a central question to direct your search. Unlike a dissertation research question, this question has to be answerable without collecting original data. You should be able to answer it based only on a review of existing publications.
Make a list of keywords
Start by creating a list of keywords related to your research topic. Include each of the key concepts or variables you’re interested in, and list any synonyms and related terms. You can add to this list if you discover new keywords in the process of your literature search.
- Social media, Facebook, Instagram, Twitter, Snapchat, TikTok
- Body image, self-perception, self-esteem, mental health
- Generation Z, teenagers, adolescents, youth
Search for relevant sources
Use your keywords to begin searching for sources. Some databases to search for journals and articles include:
- Your university’s library catalogue
- Google Scholar
- Project Muse (humanities and social sciences)
- Medline (life sciences and biomedicine)
- EconLit (economics)
- Inspec (physics, engineering and computer science)
You can use boolean operators to help narrow down your search:
Read the abstract to find out whether an article is relevant to your question. When you find a useful book or article, you can check the bibliography to find other relevant sources.
To identify the most important publications on your topic, take note of recurring citations. If the same authors, books or articles keep appearing in your reading, make sure to seek them out.
You probably won’t be able to read absolutely everything that has been written on the topic – you’ll have to evaluate which sources are most relevant to your questions.
For each publication, ask yourself:
- What question or problem is the author addressing?
- What are the key concepts and how are they defined?
- What are the key theories, models and methods? Does the research use established frameworks or take an innovative approach?
- What are the results and conclusions of the study?
- How does the publication relate to other literature in the field? Does it confirm, add to, or challenge established knowledge?
- How does the publication contribute to your understanding of the topic? What are its key insights and arguments?
- What are the strengths and weaknesses of the research?
Make sure the sources you use are credible, and make sure you read any landmark studies and major theories in your field of research.
You can find out how many times an article has been cited on Google Scholar – a high citation count means the article has been influential in the field, and should certainly be included in your literature review.
The scope of your review will depend on your topic and discipline: in the sciences you usually only review recent literature, but in the humanities you might take a long historical perspective (for example, to trace how a concept has changed in meaning over time).
Remember that you can use our template to summarise and evaluate sources you’re thinking about using!
Take notes and cite your sources
As you read, you should also begin the writing process. Take notes that you can later incorporate into the text of your literature review.
It’s important to keep track of your sources with references to avoid plagiarism . It can be helpful to make an annotated bibliography, where you compile full reference information and write a paragraph of summary and analysis for each source. This helps you remember what you read and saves time later in the process.
You can use our free APA Reference Generator for quick, correct, consistent citations.
To begin organising your literature review’s argument and structure, you need to understand the connections and relationships between the sources you’ve read. Based on your reading and notes, you can look for:
- Trends and patterns (in theory, method or results): do certain approaches become more or less popular over time?
- Themes: what questions or concepts recur across the literature?
- Debates, conflicts and contradictions: where do sources disagree?
- Pivotal publications: are there any influential theories or studies that changed the direction of the field?
- Gaps: what is missing from the literature? Are there weaknesses that need to be addressed?
This step will help you work out the structure of your literature review and (if applicable) show how your own research will contribute to existing knowledge.
- Most research has focused on young women.
- There is an increasing interest in the visual aspects of social media.
- But there is still a lack of robust research on highly-visual platforms like Instagram and Snapchat – this is a gap that you could address in your own research.
There are various approaches to organising the body of a literature review. You should have a rough idea of your strategy before you start writing.
Depending on the length of your literature review, you can combine several of these strategies (for example, your overall structure might be thematic, but each theme is discussed chronologically).
Chronological
The simplest approach is to trace the development of the topic over time. However, if you choose this strategy, be careful to avoid simply listing and summarising sources in order.
Try to analyse patterns, turning points and key debates that have shaped the direction of the field. Give your interpretation of how and why certain developments occurred.
If you have found some recurring central themes, you can organise your literature review into subsections that address different aspects of the topic.
For example, if you are reviewing literature about inequalities in migrant health outcomes, key themes might include healthcare policy, language barriers, cultural attitudes, legal status, and economic access.
Methodological
If you draw your sources from different disciplines or fields that use a variety of research methods , you might want to compare the results and conclusions that emerge from different approaches. For example:
- Look at what results have emerged in qualitative versus quantitative research
- Discuss how the topic has been approached by empirical versus theoretical scholarship
- Divide the literature into sociological, historical, and cultural sources
Theoretical
A literature review is often the foundation for a theoretical framework . You can use it to discuss various theories, models, and definitions of key concepts.
You might argue for the relevance of a specific theoretical approach, or combine various theoretical concepts to create a framework for your research.
Like any other academic text, your literature review should have an introduction , a main body, and a conclusion . What you include in each depends on the objective of your literature review.
The introduction should clearly establish the focus and purpose of the literature review.
If you are writing the literature review as part of your dissertation or thesis, reiterate your central problem or research question and give a brief summary of the scholarly context. You can emphasise the timeliness of the topic (“many recent studies have focused on the problem of x”) or highlight a gap in the literature (“while there has been much research on x, few researchers have taken y into consideration”).
Depending on the length of your literature review, you might want to divide the body into subsections. You can use a subheading for each theme, time period, or methodological approach.
As you write, make sure to follow these tips:
- Summarise and synthesise: give an overview of the main points of each source and combine them into a coherent whole.
- Analyse and interpret: don’t just paraphrase other researchers – add your own interpretations, discussing the significance of findings in relation to the literature as a whole.
- Critically evaluate: mention the strengths and weaknesses of your sources.
- Write in well-structured paragraphs: use transitions and topic sentences to draw connections, comparisons and contrasts.
In the conclusion, you should summarise the key findings you have taken from the literature and emphasise their significance.
If the literature review is part of your dissertation or thesis, reiterate how your research addresses gaps and contributes new knowledge, or discuss how you have drawn on existing theories and methods to build a framework for your research. This can lead directly into your methodology section.
A literature review is a survey of scholarly sources (such as books, journal articles, and theses) related to a specific topic or research question .
It is often written as part of a dissertation , thesis, research paper , or proposal .
There are several reasons to conduct a literature review at the beginning of a research project:
- To familiarise yourself with the current state of knowledge on your topic
- To ensure that you’re not just repeating what others have already done
- To identify gaps in knowledge and unresolved problems that your research can address
- To develop your theoretical framework and methodology
- To provide an overview of the key findings and debates on the topic
Writing the literature review shows your reader how your work relates to existing research and what new insights it will contribute.
The literature review usually comes near the beginning of your dissertation . After the introduction , it grounds your research in a scholarly field and leads directly to your theoretical framework or methodology .
Cite this Scribbr article
If you want to cite this source, you can copy and paste the citation or click the ‘Cite this Scribbr article’ button to automatically add the citation to our free Reference Generator.
McCombes, S. (2022, June 07). What is a Literature Review? | Guide, Template, & Examples. Scribbr. Retrieved 6 May 2024, from https://www.scribbr.co.uk/thesis-dissertation/literature-review/
Is this article helpful?

Shona McCombes
Other students also liked, how to write a dissertation proposal | a step-by-step guide, what is a theoretical framework | a step-by-step guide, what is a research methodology | steps & tips.
Thank you for visiting nature.com. You are using a browser version with limited support for CSS. To obtain the best experience, we recommend you use a more up to date browser (or turn off compatibility mode in Internet Explorer). In the meantime, to ensure continued support, we are displaying the site without styles and JavaScript.
- View all journals
- Explore content
- About the journal
- Publish with us
- Sign up for alerts
- CAREER FEATURE
- 04 December 2020
- Correction 09 December 2020
How to write a superb literature review
Andy Tay is a freelance writer based in Singapore.
You can also search for this author in PubMed Google Scholar
Literature reviews are important resources for scientists. They provide historical context for a field while offering opinions on its future trajectory. Creating them can provide inspiration for one’s own research, as well as some practice in writing. But few scientists are trained in how to write a review — or in what constitutes an excellent one. Even picking the appropriate software to use can be an involved decision (see ‘Tools and techniques’). So Nature asked editors and working scientists with well-cited reviews for their tips.
Access options
Access Nature and 54 other Nature Portfolio journals
Get Nature+, our best-value online-access subscription
24,99 € / 30 days
cancel any time
Subscribe to this journal
Receive 51 print issues and online access
185,98 € per year
only 3,65 € per issue
Rent or buy this article
Prices vary by article type
Prices may be subject to local taxes which are calculated during checkout
doi: https://doi.org/10.1038/d41586-020-03422-x
Interviews have been edited for length and clarity.
Updates & Corrections
Correction 09 December 2020 : An earlier version of the tables in this article included some incorrect details about the programs Zotero, Endnote and Manubot. These have now been corrected.
Hsing, I.-M., Xu, Y. & Zhao, W. Electroanalysis 19 , 755–768 (2007).
Article Google Scholar
Ledesma, H. A. et al. Nature Nanotechnol. 14 , 645–657 (2019).
Article PubMed Google Scholar
Brahlek, M., Koirala, N., Bansal, N. & Oh, S. Solid State Commun. 215–216 , 54–62 (2015).
Choi, Y. & Lee, S. Y. Nature Rev. Chem . https://doi.org/10.1038/s41570-020-00221-w (2020).
Download references
Related Articles

- Research management

Hunger on campus: why US PhD students are fighting over food
Career Feature 03 MAY 24

US National Academies report outlines barriers and solutions for scientist carers
Career News 02 MAY 24

My PI yelled at me and I’m devastated. What do I do?
Career Feature 02 MAY 24

France’s research mega-campus faces leadership crisis
News 03 MAY 24

Plagiarism in peer-review reports could be the ‘tip of the iceberg’
Nature Index 01 MAY 24

Mount Etna’s spectacular smoke rings and more — April’s best science images

How reliable is this research? Tool flags papers discussed on PubPeer
News 29 APR 24
Young talents in the fields of natural science and engineering technology
Apply for the 2024 Science Fund Program for Distinguished Young Scholars of the National Natural Science Foundation of China (Overseas).
Shenyang, Liaoning, China
Northeastern University, China
Calling for Application! Tsinghua Shenzhen International Graduate School Global Recruitment
To reshape graduate education as well as research and development to better serve local, national, regional, and global sustainable development.
Shenzhen, Guangdong, China
Tsinghua Shenzhen International Graduate School
Chief Editor, Physical Review X
The Chief Editor of PRX, you will build on this reputation and shape the journal’s scope and direction for the future.
United States (US) - Remote
American Physical Society
Assistant/Associate Professor, New York University Grossman School of Medicine
The Department of Biochemistry and Molecular Pharmacology at the NYUGSoM in Manhattan invite applications for tenure-track positions.
New York (US)
NYU Langone Health
Deputy Director. OSP
The NIH Office of Science Policy (OSP) is seeking an expert candidate to be its next Deputy Director. OSP is the agency’s central policy office an...
Bethesda, Maryland (US)
National Institutes of Health/Office of Science Policy (OSP)
Sign up for the Nature Briefing newsletter — what matters in science, free to your inbox daily.
Quick links
- Explore articles by subject
- Guide to authors
- Editorial policies
Literature Review Example/Sample
Detailed Walkthrough + Free Literature Review Template
If you’re working on a dissertation or thesis and are looking for an example of a strong literature review chapter , you’ve come to the right place.
In this video, we walk you through an A-grade literature review from a dissertation that earned full distinction . We start off by discussing the five core sections of a literature review chapter by unpacking our free literature review template . This includes:
- The literature review opening/ introduction section
- The theoretical framework (or foundation of theory)
- The empirical research
- The research gap
- The closing section
We then progress to the sample literature review (from an A-grade Master’s-level dissertation) to show how these concepts are applied in the literature review chapter. You can access the free resources mentioned in this video below.
PS – If you’re working on a dissertation, be sure to also check out our collection of dissertation and thesis examples here .
FAQ: Literature Review Example
Literature review example: frequently asked questions, is the sample literature review real.
Yes. The literature review example is an extract from a Master’s-level dissertation for an MBA program. It has not been edited in any way.
Can I replicate this literature review for my dissertation?
As we discuss in the video, every literature review will be slightly different, depending on the university’s unique requirements, as well as the nature of the research itself. Therefore, you’ll need to tailor your literature review to suit your specific context.
You can learn more about the basics of writing a literature review here .
Where can I find more examples of literature reviews?
The best place to find more examples of literature review chapters would be within dissertation/thesis databases. These databases include dissertations, theses and research projects that have successfully passed the assessment criteria for the respective university, meaning that you have at least some sort of quality assurance.
The Open Access Thesis Database (OATD) is a good starting point.
How do I get the literature review template?
You can access our free literature review chapter template here .
Is the template really free?
Yes. There is no cost for the template and you are free to use it as you wish.

Psst… there’s more!
This post is an extract from our bestselling short course, Literature Review Bootcamp . If you want to work smart, you don't want to miss this .
You Might Also Like:

What will it take for you to guide me in my Ph.D research work?
Submit a Comment Cancel reply
Your email address will not be published. Required fields are marked *
Save my name, email, and website in this browser for the next time I comment.
- Print Friendly
15 Literature Review Examples

Literature reviews are a necessary step in a research process and often required when writing your research proposal . They involve gathering, analyzing, and evaluating existing knowledge about a topic in order to find gaps in the literature where future studies will be needed.
Ideally, once you have completed your literature review, you will be able to identify how your research project can build upon and extend existing knowledge in your area of study.
Generally, for my undergraduate research students, I recommend a narrative review, where themes can be generated in order for the students to develop sufficient understanding of the topic so they can build upon the themes using unique methods or novel research questions.
If you’re in the process of writing a literature review, I have developed a literature review template for you to use – it’s a huge time-saver and walks you through how to write a literature review step-by-step:
Get your time-saving templates here to write your own literature review.
Literature Review Examples
For the following types of literature review, I present an explanation and overview of the type, followed by links to some real-life literature reviews on the topics.
1. Narrative Review Examples
Also known as a traditional literature review, the narrative review provides a broad overview of the studies done on a particular topic.
It often includes both qualitative and quantitative studies and may cover a wide range of years.
The narrative review’s purpose is to identify commonalities, gaps, and contradictions in the literature .
I recommend to my students that they should gather their studies together, take notes on each study, then try to group them by themes that form the basis for the review (see my step-by-step instructions at the end of the article).
Example Study
Title: Communication in healthcare: a narrative review of the literature and practical recommendations
Citation: Vermeir, P., Vandijck, D., Degroote, S., Peleman, R., Verhaeghe, R., Mortier, E., … & Vogelaers, D. (2015). Communication in healthcare: a narrative review of the literature and practical recommendations. International journal of clinical practice , 69 (11), 1257-1267.
Source: https://onlinelibrary.wiley.com/doi/pdf/10.1111/ijcp.12686
Overview: This narrative review analyzed themes emerging from 69 articles about communication in healthcare contexts. Five key themes were found in the literature: poor communication can lead to various negative outcomes, discontinuity of care, compromise of patient safety, patient dissatisfaction, and inefficient use of resources. After presenting the key themes, the authors recommend that practitioners need to approach healthcare communication in a more structured way, such as by ensuring there is a clear understanding of who is in charge of ensuring effective communication in clinical settings.
Other Examples
- Burnout in United States Healthcare Professionals: A Narrative Review (Reith, 2018) – read here
- Examining the Presence, Consequences, and Reduction of Implicit Bias in Health Care: A Narrative Review (Zestcott, Blair & Stone, 2016) – read here
- A Narrative Review of School-Based Physical Activity for Enhancing Cognition and Learning (Mavilidi et al., 2018) – read here
- A narrative review on burnout experienced by medical students and residents (Dyrbye & Shanafelt, 2015) – read here
2. Systematic Review Examples
This type of literature review is more structured and rigorous than a narrative review. It involves a detailed and comprehensive plan and search strategy derived from a set of specified research questions.
The key way you’d know a systematic review compared to a narrative review is in the methodology: the systematic review will likely have a very clear criteria for how the studies were collected, and clear explanations of exclusion/inclusion criteria.
The goal is to gather the maximum amount of valid literature on the topic, filter out invalid or low-quality reviews, and minimize bias. Ideally, this will provide more reliable findings, leading to higher-quality conclusions and recommendations for further research.
You may note from the examples below that the ‘method’ sections in systematic reviews tend to be much more explicit, often noting rigid inclusion/exclusion criteria and exact keywords used in searches.
Title: The importance of food naturalness for consumers: Results of a systematic review
Citation: Roman, S., Sánchez-Siles, L. M., & Siegrist, M. (2017). The importance of food naturalness for consumers: Results of a systematic review. Trends in food science & technology , 67 , 44-57.
Source: https://www.sciencedirect.com/science/article/pii/S092422441730122X
Overview: This systematic review included 72 studies of food naturalness to explore trends in the literature about its importance for consumers. Keywords used in the data search included: food, naturalness, natural content, and natural ingredients. Studies were included if they examined consumers’ preference for food naturalness and contained empirical data. The authors found that the literature lacks clarity about how naturalness is defined and measured, but also found that food consumption is significantly influenced by perceived naturalness of goods.
- A systematic review of research on online teaching and learning from 2009 to 2018 (Martin, Sun & Westine, 2020) – read here
- Where Is Current Research on Blockchain Technology? (Yli-Huumo et al., 2016) – read here
- Universities—industry collaboration: A systematic review (Ankrah & Al-Tabbaa, 2015) – read here
- Internet of Things Applications: A Systematic Review (Asghari, Rahmani & Javadi, 2019) – read here
3. Meta-analysis
This is a type of systematic review that uses statistical methods to combine and summarize the results of several studies.
Due to its robust methodology, a meta-analysis is often considered the ‘gold standard’ of secondary research , as it provides a more precise estimate of a treatment effect than any individual study contributing to the pooled analysis.
Furthermore, by aggregating data from a range of studies, a meta-analysis can identify patterns, disagreements, or other interesting relationships that may have been hidden in individual studies.
This helps to enhance the generalizability of findings, making the conclusions drawn from a meta-analysis particularly powerful and informative for policy and practice.
Title: Cholesterol and Alzheimer’s Disease Risk: A Meta-Meta-Analysis
Citation: Sáiz-Vazquez, O., Puente-Martínez, A., Ubillos-Landa, S., Pacheco-Bonrostro, J., & Santabárbara, J. (2020). Cholesterol and Alzheimer’s disease risk: a meta-meta-analysis. Brain sciences, 10(6), 386.
Source: https://doi.org/10.3390/brainsci10060386
O verview: This study examines the relationship between cholesterol and Alzheimer’s disease (AD). Researchers conducted a systematic search of meta-analyses and reviewed several databases, collecting 100 primary studies and five meta-analyses to analyze the connection between cholesterol and Alzheimer’s disease. They find that the literature compellingly demonstrates that low-density lipoprotein cholesterol (LDL-C) levels significantly influence the development of Alzheimer’s disease.
- The power of feedback revisited: A meta-analysis of educational feedback research (Wisniewski, Zierer & Hattie, 2020) – read here
- How Much Does Education Improve Intelligence? A Meta-Analysis (Ritchie & Tucker-Drob, 2018) – read here
- A meta-analysis of factors related to recycling (Geiger et al., 2019) – read here
- Stress management interventions for police officers and recruits (Patterson, Chung & Swan, 2014) – read here
Other Types of Reviews
- Scoping Review: This type of review is used to map the key concepts underpinning a research area and the main sources and types of evidence available. It can be undertaken as stand-alone projects in their own right, or as a precursor to a systematic review.
- Rapid Review: This type of review accelerates the systematic review process in order to produce information in a timely manner. This is achieved by simplifying or omitting stages of the systematic review process.
- Integrative Review: This review method is more inclusive than others, allowing for the simultaneous inclusion of experimental and non-experimental research. The goal is to more comprehensively understand a particular phenomenon.
- Critical Review: This is similar to a narrative review but requires a robust understanding of both the subject and the existing literature. In a critical review, the reviewer not only summarizes the existing literature, but also evaluates its strengths and weaknesses. This is common in the social sciences and humanities .
- State-of-the-Art Review: This considers the current level of advancement in a field or topic and makes recommendations for future research directions. This type of review is common in technological and scientific fields but can be applied to any discipline.
How to Write a Narrative Review (Tips for Undergrad Students)
Most undergraduate students conducting a capstone research project will be writing narrative reviews. Below is a five-step process for conducting a simple review of the literature for your project.
- Search for Relevant Literature: Use scholarly databases related to your field of study, provided by your university library, along with appropriate search terms to identify key scholarly articles that have been published on your topic.
- Evaluate and Select Sources: Filter the source list by selecting studies that are directly relevant and of sufficient quality, considering factors like credibility , objectivity, accuracy, and validity.
- Analyze and Synthesize: Review each source and summarize the main arguments in one paragraph (or more, for postgrad). Keep these summaries in a table.
- Identify Themes: With all studies summarized, group studies that share common themes, such as studies that have similar findings or methodologies.
- Write the Review: Write your review based upon the themes or subtopics you have identified. Give a thorough overview of each theme, integrating source data, and conclude with a summary of the current state of knowledge then suggestions for future research based upon your evaluation of what is lacking in the literature.
Literature reviews don’t have to be as scary as they seem. Yes, they are difficult and require a strong degree of comprehension of academic studies. But it can be feasibly done through following a structured approach to data collection and analysis. With my undergraduate research students (who tend to conduct small-scale qualitative studies ), I encourage them to conduct a narrative literature review whereby they can identify key themes in the literature. Within each theme, students can critique key studies and their strengths and limitations , in order to get a lay of the land and come to a point where they can identify ways to contribute new insights to the existing academic conversation on their topic.
Ankrah, S., & Omar, A. T. (2015). Universities–industry collaboration: A systematic review. Scandinavian Journal of Management, 31(3), 387-408.
Asghari, P., Rahmani, A. M., & Javadi, H. H. S. (2019). Internet of Things applications: A systematic review. Computer Networks , 148 , 241-261.
Dyrbye, L., & Shanafelt, T. (2016). A narrative review on burnout experienced by medical students and residents. Medical education , 50 (1), 132-149.
Geiger, J. L., Steg, L., Van Der Werff, E., & Ünal, A. B. (2019). A meta-analysis of factors related to recycling. Journal of environmental psychology , 64 , 78-97.
Martin, F., Sun, T., & Westine, C. D. (2020). A systematic review of research on online teaching and learning from 2009 to 2018. Computers & education , 159 , 104009.
Mavilidi, M. F., Ruiter, M., Schmidt, M., Okely, A. D., Loyens, S., Chandler, P., & Paas, F. (2018). A narrative review of school-based physical activity for enhancing cognition and learning: The importance of relevancy and integration. Frontiers in psychology , 2079.
Patterson, G. T., Chung, I. W., & Swan, P. W. (2014). Stress management interventions for police officers and recruits: A meta-analysis. Journal of experimental criminology , 10 , 487-513.
Reith, T. P. (2018). Burnout in United States healthcare professionals: a narrative review. Cureus , 10 (12).
Ritchie, S. J., & Tucker-Drob, E. M. (2018). How much does education improve intelligence? A meta-analysis. Psychological science , 29 (8), 1358-1369.
Roman, S., Sánchez-Siles, L. M., & Siegrist, M. (2017). The importance of food naturalness for consumers: Results of a systematic review. Trends in food science & technology , 67 , 44-57.
Sáiz-Vazquez, O., Puente-Martínez, A., Ubillos-Landa, S., Pacheco-Bonrostro, J., & Santabárbara, J. (2020). Cholesterol and Alzheimer’s disease risk: a meta-meta-analysis. Brain sciences, 10(6), 386.
Vermeir, P., Vandijck, D., Degroote, S., Peleman, R., Verhaeghe, R., Mortier, E., … & Vogelaers, D. (2015). Communication in healthcare: a narrative review of the literature and practical recommendations. International journal of clinical practice , 69 (11), 1257-1267.
Wisniewski, B., Zierer, K., & Hattie, J. (2020). The power of feedback revisited: A meta-analysis of educational feedback research. Frontiers in Psychology , 10 , 3087.
Yli-Huumo, J., Ko, D., Choi, S., Park, S., & Smolander, K. (2016). Where is current research on blockchain technology?—a systematic review. PloS one , 11 (10), e0163477.
Zestcott, C. A., Blair, I. V., & Stone, J. (2016). Examining the presence, consequences, and reduction of implicit bias in health care: a narrative review. Group Processes & Intergroup Relations , 19 (4), 528-542

Chris Drew (PhD)
Dr. Chris Drew is the founder of the Helpful Professor. He holds a PhD in education and has published over 20 articles in scholarly journals. He is the former editor of the Journal of Learning Development in Higher Education. [Image Descriptor: Photo of Chris]
- Chris Drew (PhD) https://helpfulprofessor.com/author/chris-drew-phd/ What is Educational Psychology?
- Chris Drew (PhD) https://helpfulprofessor.com/author/chris-drew-phd/ What is IQ? (Intelligence Quotient)
- Chris Drew (PhD) https://helpfulprofessor.com/author/chris-drew-phd/ 5 Top Tips for Succeeding at University
- Chris Drew (PhD) https://helpfulprofessor.com/author/chris-drew-phd/ 50 Durable Goods Examples
Leave a Comment Cancel Reply
Your email address will not be published. Required fields are marked *
How to write a literature review introduction (+ examples)

The introduction to a literature review serves as your reader’s guide through your academic work and thought process. Explore the significance of literature review introductions in review papers, academic papers, essays, theses, and dissertations. We delve into the purpose and necessity of these introductions, explore the essential components of literature review introductions, and provide step-by-step guidance on how to craft your own, along with examples.
Why you need an introduction for a literature review
When you need an introduction for a literature review, what to include in a literature review introduction, examples of literature review introductions, steps to write your own literature review introduction.
A literature review is a comprehensive examination of the international academic literature concerning a particular topic. It involves summarizing published works, theories, and concepts while also highlighting gaps and offering critical reflections.
In academic writing , the introduction for a literature review is an indispensable component. Effective academic writing requires proper paragraph structuring to guide your reader through your argumentation. This includes providing an introduction to your literature review.
It is imperative to remember that you should never start sharing your findings abruptly. Even if there isn’t a dedicated introduction section .
Instead, you should always offer some form of introduction to orient the reader and clarify what they can expect.
There are three main scenarios in which you need an introduction for a literature review:
- Academic literature review papers: When your literature review constitutes the entirety of an academic review paper, a more substantial introduction is necessary. This introduction should resemble the standard introduction found in regular academic papers.
- Literature review section in an academic paper or essay: While this section tends to be brief, it’s important to precede the detailed literature review with a few introductory sentences. This helps orient the reader before delving into the literature itself.
- Literature review chapter or section in your thesis/dissertation: Every thesis and dissertation includes a literature review component, which also requires a concise introduction to set the stage for the subsequent review.
You may also like: How to write a fantastic thesis introduction (+15 examples)
It is crucial to customize the content and depth of your literature review introduction according to the specific format of your academic work.
In practical terms, this implies, for instance, that the introduction in an academic literature review paper, especially one derived from a systematic literature review , is quite comprehensive. Particularly compared to the rather brief one or two introductory sentences that are often found at the beginning of a literature review section in a standard academic paper. The introduction to the literature review chapter in a thesis or dissertation again adheres to different standards.
Here’s a structured breakdown based on length and the necessary information:
Academic literature review paper
The introduction of an academic literature review paper, which does not rely on empirical data, often necessitates a more extensive introduction than the brief literature review introductions typically found in empirical papers. It should encompass:
- The research problem: Clearly articulate the problem or question that your literature review aims to address.
- The research gap: Highlight the existing gaps, limitations, or unresolved aspects within the current body of literature related to the research problem.
- The research relevance: Explain why the chosen research problem and its subsequent investigation through a literature review are significant and relevant in your academic field.
- The literature review method: If applicable, describe the methodology employed in your literature review, especially if it is a systematic review or follows a specific research framework.
- The main findings or insights of the literature review: Summarize the key discoveries, insights, or trends that have emerged from your comprehensive review of the literature.
- The main argument of the literature review: Conclude the introduction by outlining the primary argument or statement that your literature review will substantiate, linking it to the research problem and relevance you’ve established.
- Preview of the literature review’s structure: Offer a glimpse into the organization of the literature review paper, acting as a guide for the reader. This overview outlines the subsequent sections of the paper and provides an understanding of what to anticipate.
By addressing these elements, your introduction will provide a clear and structured overview of what readers can expect in your literature review paper.
Regular literature review section in an academic article or essay
Most academic articles or essays incorporate regular literature review sections, often placed after the introduction. These sections serve to establish a scholarly basis for the research or discussion within the paper.
In a standard 8000-word journal article, the literature review section typically spans between 750 and 1250 words. The first few sentences or the first paragraph within this section often serve as an introduction. It should encompass:
- An introduction to the topic: When delving into the academic literature on a specific topic, it’s important to provide a smooth transition that aids the reader in comprehending why certain aspects will be discussed within your literature review.
- The core argument: While literature review sections primarily synthesize the work of other scholars, they should consistently connect to your central argument. This central argument serves as the crux of your message or the key takeaway you want your readers to retain. By positioning it at the outset of the literature review section and systematically substantiating it with evidence, you not only enhance reader comprehension but also elevate overall readability. This primary argument can typically be distilled into 1-2 succinct sentences.
In some cases, you might include:
- Methodology: Details about the methodology used, but only if your literature review employed a specialized method. If your approach involved a broader overview without a systematic methodology, you can omit this section, thereby conserving word count.
By addressing these elements, your introduction will effectively integrate your literature review into the broader context of your academic paper or essay. This will, in turn, assist your reader in seamlessly following your overarching line of argumentation.
Introduction to a literature review chapter in thesis or dissertation
The literature review typically constitutes a distinct chapter within a thesis or dissertation. Often, it is Chapter 2 of a thesis or dissertation.
Some students choose to incorporate a brief introductory section at the beginning of each chapter, including the literature review chapter. Alternatively, others opt to seamlessly integrate the introduction into the initial sentences of the literature review itself. Both approaches are acceptable, provided that you incorporate the following elements:
- Purpose of the literature review and its relevance to the thesis/dissertation research: Explain the broader objectives of the literature review within the context of your research and how it contributes to your thesis or dissertation. Essentially, you’re telling the reader why this literature review is important and how it fits into the larger scope of your academic work.
- Primary argument: Succinctly communicate what you aim to prove, explain, or explore through the review of existing literature. This statement helps guide the reader’s understanding of the review’s purpose and what to expect from it.
- Preview of the literature review’s content: Provide a brief overview of the topics or themes that your literature review will cover. It’s like a roadmap for the reader, outlining the main areas of focus within the review. This preview can help the reader anticipate the structure and organization of your literature review.
- Methodology: If your literature review involved a specific research method, such as a systematic review or meta-analysis, you should briefly describe that methodology. However, this is not always necessary, especially if your literature review is more of a narrative synthesis without a distinct research method.
By addressing these elements, your introduction will empower your literature review to play a pivotal role in your thesis or dissertation research. It will accomplish this by integrating your research into the broader academic literature and providing a solid theoretical foundation for your work.
Comprehending the art of crafting your own literature review introduction becomes significantly more accessible when you have concrete examples to examine. Here, you will find several examples that meet, or in most cases, adhere to the criteria described earlier.
Example 1: An effective introduction for an academic literature review paper
To begin, let’s delve into the introduction of an academic literature review paper. We will examine the paper “How does culture influence innovation? A systematic literature review”, which was published in 2018 in the journal Management Decision.
The entire introduction spans 611 words and is divided into five paragraphs. In this introduction, the authors accomplish the following:
- In the first paragraph, the authors introduce the broader topic of the literature review, which focuses on innovation and its significance in the context of economic competition. They underscore the importance of this topic, highlighting its relevance for both researchers and policymakers.
- In the second paragraph, the authors narrow down their focus to emphasize the specific role of culture in relation to innovation.
- In the third paragraph, the authors identify research gaps, noting that existing studies are often fragmented and disconnected. They then emphasize the value of conducting a systematic literature review to enhance our understanding of the topic.
- In the fourth paragraph, the authors introduce their specific objectives and explain how their insights can benefit other researchers and business practitioners.
- In the fifth and final paragraph, the authors provide an overview of the paper’s organization and structure.
In summary, this introduction stands as a solid example. While the authors deviate from previewing their key findings (which is a common practice at least in the social sciences), they do effectively cover all the other previously mentioned points.
Example 2: An effective introduction to a literature review section in an academic paper
The second example represents a typical academic paper, encompassing not only a literature review section but also empirical data, a case study, and other elements. We will closely examine the introduction to the literature review section in the paper “The environmentalism of the subalterns: a case study of environmental activism in Eastern Kurdistan/Rojhelat”, which was published in 2021 in the journal Local Environment.
The paper begins with a general introduction and then proceeds to the literature review, designated by the authors as their conceptual framework. Of particular interest is the first paragraph of this conceptual framework, comprising 142 words across five sentences:
“ A peripheral and marginalised nationality within a multinational though-Persian dominated Iranian society, the Kurdish people of Iranian Kurdistan (a region referred by the Kurds as Rojhelat/Eastern Kurdi-stan) have since the early twentieth century been subject to multifaceted and systematic discriminatory and exclusionary state policy in Iran. This condition has left a population of 12–15 million Kurds in Iran suffering from structural inequalities, disenfranchisement and deprivation. Mismanagement of Kurdistan’s natural resources and the degradation of its natural environmental are among examples of this disenfranchisement. As asserted by Julian Agyeman (2005), structural inequalities that sustain the domination of political and economic elites often simultaneously result in environmental degradation, injustice and discrimination against subaltern communities. This study argues that the environmental struggle in Eastern Kurdistan can be asserted as a (sub)element of the Kurdish liberation movement in Iran. Conceptually this research is inspired by and has been conducted through the lens of ‘subalternity’ ” ( Hassaniyan, 2021, p. 931 ).
In this first paragraph, the author is doing the following:
- The author contextualises the research
- The author links the research focus to the international literature on structural inequalities
- The author clearly presents the argument of the research
- The author clarifies how the research is inspired by and uses the concept of ‘subalternity’.
Thus, the author successfully introduces the literature review, from which point onward it dives into the main concept (‘subalternity’) of the research, and reviews the literature on socio-economic justice and environmental degradation.
While introductions to a literature review section aren’t always required to offer the same level of study context detail as demonstrated here, this introduction serves as a commendable model for orienting the reader within the literature review. It effectively underscores the literature review’s significance within the context of the study being conducted.
Examples 3-5: Effective introductions to literature review chapters
The introduction to a literature review chapter can vary in length, depending largely on the overall length of the literature review chapter itself. For example, a master’s thesis typically features a more concise literature review, thus necessitating a shorter introduction. In contrast, a Ph.D. thesis, with its more extensive literature review, often includes a more detailed introduction.
Numerous universities offer online repositories where you can access theses and dissertations from previous years, serving as valuable sources of reference. Many of these repositories, however, may require you to log in through your university account. Nevertheless, a few open-access repositories are accessible to anyone, such as the one by the University of Manchester . It’s important to note though that copyright restrictions apply to these resources, just as they would with published papers.
Master’s thesis literature review introduction
The first example is “Benchmarking Asymmetrical Heating Models of Spider Pulsar Companions” by P. Sun, a master’s thesis completed at the University of Manchester on January 9, 2024. The author, P. Sun, introduces the literature review chapter very briefly but effectively:
PhD thesis literature review chapter introduction
The second example is Deep Learning on Semi-Structured Data and its Applications to Video-Game AI, Woof, W. (Author). 31 Dec 2020, a PhD thesis completed at the University of Manchester . In Chapter 2, the author offers a comprehensive introduction to the topic in four paragraphs, with the final paragraph serving as an overview of the chapter’s structure:
PhD thesis literature review introduction
The last example is the doctoral thesis Metacognitive strategies and beliefs: Child correlates and early experiences Chan, K. Y. M. (Author). 31 Dec 2020 . The author clearly conducted a systematic literature review, commencing the review section with a discussion of the methodology and approach employed in locating and analyzing the selected records.
Having absorbed all of this information, let’s recap the essential steps and offer a succinct guide on how to proceed with creating your literature review introduction:
- Contextualize your review : Begin by clearly identifying the academic context in which your literature review resides and determining the necessary information to include.
- Outline your structure : Develop a structured outline for your literature review, highlighting the essential information you plan to incorporate in your introduction.
- Literature review process : Conduct a rigorous literature review, reviewing and analyzing relevant sources.
- Summarize and abstract : After completing the review, synthesize the findings and abstract key insights, trends, and knowledge gaps from the literature.
- Craft the introduction : Write your literature review introduction with meticulous attention to the seamless integration of your review into the larger context of your work. Ensure that your introduction effectively elucidates your rationale for the chosen review topics and the underlying reasons guiding your selection.

Master Academia
Get new content delivered directly to your inbox.
Subscribe and receive Master Academia's quarterly newsletter.
The best answers to "What are your plans for the future?"
10 tips for engaging your audience in academic writing, related articles.

10 key skills of successful master’s students
How to write effective cover letters for a paper submission

Dealing with failure as a PhD student

Reject decisions: Sample peer review comments and examples
Literature Reviews
- "How To" Books
- Examples of Literature Reviews
- Collecting Resources for a Literature Review
- Organizing the Literature Review
- Writing the Literature Review
- Endnote This link opens in a new window
- Evaluating Websites
Examples of Literature Reviews in Government Document and Book Format
- Social and economic considerations for coastal and watershed restoration in the Puget Sound, Washington : a literature review by Holly M. Stinchfield, Lynne Koontz, and Natalie R. Sexton Call Number: U.S. Government Documents Online
- A literature review of wipe sampling methods for chemical warfare agents and toxic industrial chemicals by Battelle Call Number: U.S.Government Documents Online Washington, DC : Office of Research and Development, U.S. Environmental Protection Agency, [2007]
- Collaboration, technology, and outsourcing initiatives in higher education : a literature review by Tessa Kaganoff. Call Number: ebook Santa Monica, CA : RAND, 1998

Examples of Literature Reviews in Journal Articles and Disserations
- The stigma of childhood obesity: A literature review by Janel Swaye MacDermott
Journal Articles
Papastergiou, Marina. 2009. "Exploring the potential of computer and video games for health and physical education: A literature review." Computers & Education 53, no. 3: 603-622.
de Campos, Ana Carolina, Nelci Adriana Cicuto Ferreira Rocha, and Geert J. P. Savelsbergh. "Reaching and grasping movements in infants at risk: A review." Research in Developmental Disabilities 30, no. 5 (September 2009): 819-826.
Dissertations
- A meta-analysis/literature review comparing the effectiveness of SSRI antidepressants, cognitive behavioral therapy, and placebo for the treatment of depression by John J Wagner
- << Previous: "How To" Books
- Next: Collecting Resources for a Literature Review >>
- Last Updated: Nov 2, 2021 12:11 PM
- URL: https://guides.library.stonybrook.edu/literature-review
- Request a Class
- Hours & Locations
- Ask a Librarian
- Special Collections
- Library Faculty & Staff
Library Administration: 631.632.7100
- Stony Brook Home
- Campus Maps
- Web Accessibility Information
- Accessibility Barrier Report Form

Comments or Suggestions? | Library Webmaster

Except where otherwise noted, this work by SBU Libraries is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License .

Guide to Thematic Analysis

- Abductive Thematic Analysis
- Collaborative Thematic Analysis
- Deductive Thematic Analysis
- How to Do Thematic Analysis
- Inductive Thematic Analysis
- Reflexive Thematic Analysis
- Advantages of Thematic Analysis
- Thematic Analysis for Case Studies
- Thematic Coding
- Disadvantages of Thematic Analysis
- Thematic Analysis in Educational Research
- Thematic Analysis Examples
- Thematic Analysis for Focus Groups
- Thematic Analysis vs. Grounded Theory
- What is Thematic Analysis?
- Increasing Rigor in Thematic Analysis
- Thematic Analysis for Interviews
- Introduction
What is a thematic literature review?
Advantages of a thematic literature review, structuring and writing a thematic literature review.
- Thematic Analysis in Mixed Methods Approach
- Thematic Analysis in Observations
- Peer Review in Thematic Analysis
- How to Present Thematic Analysis Results
- Thematic Analysis in Psychology
- Thematic Analysis of Secondary Data
- Thematic Analysis in Social Work
- Thematic Analysis Software
- Thematic Analysis in Surveys
- Thematic Analysis in UX Research
- Thematic vs. Content Analysis
- Thematic Analysis vs. Discourse Analysis
- Thematic Analysis vs. Framework Analysis
- Thematic Analysis vs. Narrative Analysis
- Thematic Analysis vs. Phenomenology
Thematic Analysis Literature Review
A thematic literature review serves as a critical tool for synthesizing research findings within a specific subject area. By categorizing existing literature into themes, this method offers a structured approach to identify and analyze patterns and trends across studies. The primary goal is to provide a clear and concise overview that aids scholars and practitioners in understanding the key discussions and developments within a field. Unlike traditional literature reviews , which may adopt a chronological approach or focus on individual studies, a thematic literature review emphasizes the aggregation of findings through key themes and thematic connections. This introduction sets the stage for a detailed examination of what constitutes a thematic literature review, its benefits, and guidance on effectively structuring and writing one.

A thematic literature review methodically organizes and examines a body of literature by identifying, analyzing, and reporting themes found within texts such as journal articles, conference proceedings, dissertations, and other forms of academic writing. While a particular journal article may offer some specific insight, a synthesis of knowledge through a literature review can provide a comprehensive overview of theories across relevant sources in a particular field.
Unlike other review types that might organize literature chronologically or by methodology , a thematic review focuses on recurring themes or patterns across a collection of works. This approach enables researchers to draw together previous research to synthesize findings from different research contexts and methodologies, highlighting the overarching trends and insights within a field.
At its core, a thematic approach to a literature review research project involves several key steps. Initially, it requires the comprehensive collection of relevant literature that aligns with the review's research question or objectives. Following this, the process entails a meticulous analysis of the texts to identify common themes that emerge across the studies. These themes are not pre-defined but are discovered through a careful reading and synthesis of the literature.
The thematic analysis process is iterative, often involving the refinement of themes as the review progresses. It allows for the integration of a broad range of literature, facilitating a multidimensional understanding of the research topic. By organizing literature thematically, the review illuminates how various studies contribute to each theme, providing insights into the depth and breadth of research in the area.
A thematic literature review thus serves as a foundational element in research, offering a nuanced and comprehensive perspective on a topic. It not only aids in identifying gaps in the existing literature but also guides future research directions by underscoring areas that warrant further investigation. Ultimately, a thematic literature review empowers researchers to construct a coherent narrative that weaves together disparate studies into a unified analysis.
Organize your literature search with ATLAS.ti
Collect and categorize documents to identify gaps and key findings with ATLAS.ti. Download a free trial.
Conducting a literature review thematically provides a comprehensive and nuanced synthesis of research findings, distinguishing it from other types of literature reviews. Its structured approach not only facilitates a deeper understanding of the subject area but also enhances the clarity and relevance of the review. Here are three significant advantages of employing a thematic analysis in literature reviews.
Enhanced understanding of the research field
Thematic literature reviews allow for a detailed exploration of the research landscape, presenting themes that capture the essence of the subject area. By identifying and analyzing these themes, reviewers can construct a narrative that reflects the complexity and multifaceted nature of the field.
This process aids in uncovering underlying patterns and relationships, offering a more profound and insightful examination of the literature. As a result, readers gain an enriched understanding of the key concepts, debates, and evolutionary trajectories within the research area.
Identification of research gaps and trends
One of the pivotal benefits of a thematic literature review is its ability to highlight gaps in the existing body of research. By systematically organizing the literature into themes, reviewers can pinpoint areas that are under-explored or warrant further investigation.
Additionally, this method can reveal emerging trends and shifts in research focus, guiding scholars toward promising areas for future study. The thematic structure thus serves as a roadmap, directing researchers toward uncharted territories and new research questions .
Facilitates comparative analysis and integration of findings
A thematic literature review excels in synthesizing findings from diverse studies, enabling a coherent and integrated overview. By concentrating on themes rather than individual studies, the review can draw comparisons and contrasts across different research contexts and methodologies . This comparative analysis enriches the review, offering a panoramic view of the field that acknowledges both consensus and divergence among researchers.
Moreover, the thematic framework supports the integration of findings, presenting a unified and comprehensive portrayal of the research area. Such integration is invaluable for scholars seeking to navigate the extensive body of literature and extract pertinent insights relevant to their own research questions or objectives.
The process of structuring and writing a thematic literature review is pivotal in presenting research in a clear, coherent, and impactful manner. This review type necessitates a methodical approach to not only unearth and categorize key themes but also to articulate them in a manner that is both accessible and informative to the reader. The following sections outline essential stages in the thematic analysis process for literature reviews , offering a structured pathway from initial planning to the final presentation of findings.
Identifying and categorizing themes
The initial phase in a thematic literature review is the identification of themes within the collected body of literature. This involves a detailed examination of texts to discern patterns, concepts, and ideas that recur across the research landscape. Effective identification hinges on a thorough and nuanced reading of the literature, where the reviewer actively engages with the content to extract and note significant thematic elements. Once identified, these themes must be meticulously categorized, often requiring the reviewer to discern between overarching themes and more nuanced sub-themes, ensuring a logical and hierarchical organization of the review content.
Analyzing and synthesizing themes
After categorizing the themes, the next step involves a deeper analysis and synthesis of the identified themes. This stage is critical for understanding the relationships between themes and for interpreting the broader implications of the thematic findings. Analysis may reveal how themes evolve over time, differ across methodologies or contexts, or converge to highlight predominant trends in the research area. Synthesis involves integrating insights from various studies to construct a comprehensive narrative that encapsulates the thematic essence of the literature, offering new interpretations or revealing gaps in existing research.
Presenting and discussing findings
The final stage of the thematic literature review is the discussion of the thematic findings in a research paper or presentation. This entails not only a descriptive account of identified themes but also a critical examination of their significance within the research field. Each theme should be discussed in detail, elucidating its relevance, the extent of research support, and its implications for future studies. The review should culminate in a coherent and compelling narrative that not only summarizes the key thematic findings but also situates them within the broader research context, offering valuable insights and directions for future inquiry.

Gain a comprehensive understanding of your data with ATLAS.ti
Analyze qualitative data with specific themes that offer insights. See how with a free trial.
- Case report
- Open access
- Published: 02 May 2024
Cardiac evaluation in amiodarone-induced thyroid dysfunction with suspected cardiac ischemia?: a case report and review of the literature
- Yoann Aubry 1 , 2 ,
- Michel Dosch 3 &
- Marc Y. Donath 2
Journal of Medical Case Reports volume 18 , Article number: 235 ( 2024 ) Cite this article
75 Accesses
1 Altmetric
Metrics details
Amiodarone-induced thyroid dysfunction (AIT) is a side-effect associated with the use of Amiodarone for the treatment of refractory arrythmias. Resulting hyperthyroidism can precipitate cardiac complications, including cardiac ischemia and myocardial infarction, although this has only been described in a few case reports.
Case presentation
We present here a clinical scenario involving a 66-year-old male Caucasian patient under Amiodarone for atrial fibrillation, who developed AIT. In the presence of dyspnea, multiple cardiovascular risk factors and ECG abnormalities, a transthoracic echocardiogram was performed, showing inferobasal hypokinesia. This led to further investigations through a cardiac PET-CT, where cardiac ischemia was suspected. Ultimately, the coronary angiography revealed no abnormalities. Nonetheless, these extensive cardiologic investigations led to a delay in initiating an emergency endovascular revascularization for acute-on-chronic left limb ischemia. Although initial treatment using Carbimazole was not successful after three weeks, the patient reached euthyroidism after completion of the treatment with Prednisone so that eventually thyroidectomy was not performed. Endovascular revascularization was finally performed after more than one month.
Conclusions
We discuss here cardiac abnormalities in patients with AIT, which may be due to relative ischemia secondary to increased metabolic demand during hyperthyroidism. Improvement of cardiac complications is expected through an optimal AIT therapy including medical therapy as the primary approach and, when necessary, thyroidectomy. Cardiac investigations in the context of AIT should be carefully considered and may not justify delaying other crucial interventions. If considered mandatory, diagnostic procedures such as coronary angiography should be preferred to functional testing.
Peer Review reports
Introduction
Amiodarone is a class III anti-arrhythmic drug widely used in clinical practice as second-line therapy for refractory ventricular and supra-ventricular arrythmias [ 1 ]. Thyroid dysfunction under amiodarone affects up to 20% of treated patients, either hyperthyroidism/thyrotoxicosis or hypothyroidism [ 2 , 3 ]. Two types of Amiodarone-Induced Thyroid Dysfunction (AIT) are distinguished: type 1 AIT is a form of iodine-induced hyperthyroidism typically arising in a gland with underlying functional autonomy, while type 2 AIT is a destructive thyroiditis developing in a normal gland. The treatment of choice usually consists of a combination of thionamides and glucocorticoids, as distinguishing between the two types of AIT can be challenging [ 2 , 4 , 5 ]. However, resolution of hyperthyroidism takes usually several weeks to months.
Amiodarone-induced hyperthyroidism may be associated to serious cardiac complications. In particular, hyperthyroidism can lead to cardiac ischemia and even to a secondary myocardial infarction [ 6 , 7 , 8 , 9 , 10 , 11 , 12 ]. In addition, hyperthyroidism is also associated with a pro-coagulant state and can aggravate cardiac and limb ischemia [ 13 , 14 ]. Both conditions might benefit from an early thyroidectomy.
Therefore, one challenge resides in the indication and the optimal timing for the thyroidectomy. Indeed, anaesthetizing a patient with a decreased hemodynamic status or suspicion for cardiac ischemia can be challenging and the need for further investigations with the aim to mitigate potential intra- or peri-operative complications should be balanced with the delay of the thyroidectomy.
We describe here a clinical scenario with AIT, suspected cardiac ischemia and acute-on-chronic limb ischemia. Extensive cardiac investigations were carried out, which revealed false-positive functional imaging, probably due to increased cardiac metabolism, resulting in a delay in revascularization of limb ischemia. Our aim is to discuss the rationale of such investigations and the benefits of an early thyroidectomy.
Materials and methods
In accordance with ethical guidelines, written informed consent was obtained from the patient involved for the publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal. The patient's identity has been rigorously protected, and any potentially identifying information has been appropriately anonymized to ensure confidentiality and privacy.
In order to discuss the association between hyperthyroidism and cardiac ischemia, and the indication for cardiac investigations in AIT, we conducted a literature research on PubMed and MEDLINE using the following keywords: “Amiodarone-Induced Thyroid Dysfunction”, “hyperthyroidism”, “cardiac ischemia”, “thyroidectomy”. Only articles written in English were considered for this case report.
Our patient is a 66-years old male Caucasian patient known for active smoking (~ 60 pack years), hypertension and dyslipidemia, who presented with severe hyperthyroidism induced by amiodarone (given for the treatment of atrial fibrillation). At the time of diagnosis, he presented with tachycardia but no hemodynamic instability, NYHA stage 2 dyspnea and unexplained weight loss. Initial laboratory work-up showed suppressed TSH < 0.05 mUI/l, free T3 13.9 pmol/l and free T4 72 pmol/l. Anti-TSH antibodies were negative. Thyroid ultrasound showed a hypovascular thyroid and the absence of thyroid nodules. Thyreostatic treatment with Carbimazole tablets 60 mg/day was initiated. After 3 weeks, the patient was still hyperthyroid, so prednisone tablets 40 mg/day were added.
Meanwhile, the patient displayed obliterative arteriopathy of the lower limbs, stage IIA Fontaine in the left lower limb, with distal embolization of a tight stenosis of the homolateral common iliac artery, stage I Fontaine in the right lower limb. Although left limb ischemia was not critical, it required a rapid endovascular revascularization. Thyroid normalization is essential prior to vascular intervention, due to the procoagulant state associated with hyperthyroidism.
In the absence of response to drug treatment after three weeks, thyroidectomy was discussed. In this context, and due to a high cardiovascular risk associated with dyspnea, a transthoracic echocardiogram showed inferobasal hypokinesia and a cardiac PET-CT was performed, showing suspected inferobasal and inferoapical ischemia (Fig. 1 ).

Cardiac PET scan findings of our patient. No scar but evidence of infero-lateral to infero-apical ischemia (Perfusion). Localized decreased flow reserve in ischemia area. Preserved left ventricular pump function (Motilität) with normal left ventricular ejection fraction (LVEF). SRS summed rest score, SDS summed difference score, SSS summed stress score, a apical, as apico-septal, al apico-lateral, is infero-septal, il infero-lateral, i inferior
After multidisciplinary discussion involving cardiology, anesthesiology, angiology and endocrinology, it was decided to perform coronary angiography as soon as possible to rule out cardiac ischemia. Coronary angiography showed no abnormalities requiring revascularization.
Following the various cardiac investigations and the related delay, the evolution of his thyroid function was resolved after more than a month (TSH 0.91mUI/l, free T4 14.2pmol/l, free T3 3.2pmol/l) without surgery, and the patient underwent successful endovascular revascularisation for his peripheral arterial disease.
The clinical scenario presented here emphasizes a patient exhibiting amiodarone-induced hyperthyroidism, requiring prompt intervention to mitigate potential complications, including acute limb ischemia. However, concerns regarding cardiac ischemia introduced a slowdown in the treatment process. Ultimately, thyroidectomy was not performed and vascular interventions were postponed until euthyroid status was achieved. In this situation, where the treatment of hyperthyroidism and peripheral arterial disease are decisive, it is of interest to discuss the indication for additional cardiologic investigations, including cardiac PET scan. Especially considering the impact of hyperthyroidism on cardiac muscle [ 15 , 16 ], and the recent literature suggesting that patients with hyperthyroidism-related cardiac complications might benefit from an early thyroidectomy [ 17 , 18 , 19 , 20 ]. Indeed, PET scan in patients with hyperthyroidism may display false positive results for coronary artery disease due to hypermetabolism with consecutive relative ischemia.
AIT can be associated with cardiovascular complications, including rhythm disorders such as tachycardia and atrial fibrillation, along with high-output congestive heart failure, among others [ 15 , 16 ]. In more uncommon instances, it may also result in cardiac ischemia and acute myocardial infarction [ 6 , 7 , 8 , 9 , 10 , 11 , 12 ].
Thyroid hormones induce cell proliferation in the vascular wall typically leading to cardiac hypertrophy with progressively worsening high-output congestive heart failure, as evidenced by a decrease in echocardiography-measured left ventricular ejection fraction (LVEF) [ 21 ].
Cardiac Ischemia related to hyperthyroidism is rarely described in the literature and is the topic of older publications and a limited number of case reports [ 6 , 7 , 8 , 9 , 10 , 11 , 12 ]. It has been particularly described in elderly patients with coronary artery disease [ 22 ]. The mechanisms explaining cardiac ischemia in patients with hyperthyroidism remain unclear, but they might involve an increased myocardial oxygen demand related to cardiac hypertrophy, temporary coronary artery occlusion in a procoagulant state and vasoconstriction / vasospasm. Although the molecular mechanism remains unclear, there is some similarity with the clinical impact of excess catecholamines on the suffering of cardiac muscle. This may be due to thyroid hormones, which enhance the sympathetic nervous system by increasing the sensitivity of beta receptors [ 23 ] .
Indeed, hyperthyroidism is associated with a procoagulant state disrupting both primary and secondary hemostasis. Among other factors, elevation of von Willebrand factor levels with enhanced platelets function and increased factor X activity in the coagulation cascade have been described, all contributing to an elevated risk of coronary artery disease [ 13 , 14 ]. In addition, the increase of thyroid hormones seem to be associated to coronary vascular degeneration and plaque instability [ 24 ]. In our case, this also justify to treat the limb ischemia in euthyroidism.
Thyroid hormones are also known to sensitize adrenergic receptors what enhances the vasoconstrictor effect of catecholamines on coronary arteries and hyperkinetic circulation, another possible cause of cardiac ischemia [ 16 ].
The clinical presentation and concomitant medications suggest AIT. However, the exact etiology of hyperthyroidism remains unclear and amiodarone-induced destructive thyroiditis is conceivable.
Given cardio-vascular complications related to hyperthyroidism, patients will primarily benefit from prompt treatment and restoration of euthyroidism [ 21 ]. Antithyroid drugs are the first-line treatment in this case, usually a combination of thionamides and glucocorticoids [ 4 , 5 ]. Discontinuing amiodarone, which has a half-life of 100 days and acts as a T4 to T3 conversion inhibitor, is not recommended [ 2 , 4 , 5 ]. It will likely be ineffective and, even worse, might exacerbate the thyrotoxic state, potentially resulting in dangerous arrhythmias. Since medical treatment is expected to improve cardiac symptoms [ 12 ], additional cardiac investigations, such as a cardiac PET scan or a coronary angiography, should always be critically evaluated as they could potentially delay other critical interventions. A cardiac PET scan can suspect cardiac ischemia related for example to vasospasm in the coronary angiography, which can be resolved with appropriately treated hyperthyroidism [ 6 , 7 , 8 , 11 , 25 ]. However, a coronary angiography remains clearly indicated in case an acute myocardial infarction is suspected.
In line with the guidelines of the European Thyroid Association (ETA), a total or near-total thyroidectomy should then be considered for patients who do not respond to medical treatment for more than 2 weeks, exhibit a worsening cardiac status, or experience severe thyrotoxicosis requiring prompt resolution [ 20 , 26 ]. In our case, rapid resolution of hyperthyroidism was necessary to perform endovascular limb revascularization.
Although anaesthetizing a patient with hyperthyroidism or AIT can be challenging, it doesn’t appear to be associated with increased intra- or peri-operative complications [ 17 , 27 , 28 , 29 ]. However, one study described slightly elevated peri-operative morbidity and mortality [ 20 ]. Although patients are usually operated in euthyroid state, it has been shown in recent publications that patients with a mild to severe heart insufficiency for example will benefit from early thyroidectomy, in thyrotoxicosis when necessary [ 17 , 18 , 19 , 20 ]. This approach also appears reasonable, particularly when other critical operations are necessary, as in this clinical scenario a rapid endovascular revascularization. In our case, adopting a watchful-waiting strategy regarding the operation could have been associated to increased risk for complications, including exacerbation of limb ischemia.
Cardiac investigations with metabolic imaging (e.g., PET scan) in the context of AIT should not delay thyroidectomy especially when other crucial interventions are planned. A coronary angiography remains indicated in case of high suspicion of coronary stenosis or myocardial infarction. Thyroid surgery should be considered early in the treatment plan and patients might benefit from a simplified procedure.
Availability of data and materials
Data supporting our findings were taken from the patient’s folder.
Vassallo P, Trohman RG. Prescribing amiodarone: an evidence-based review of clinical indications. JAMA. 2007;298:1312–22.
Article CAS PubMed Google Scholar
Martino E, Bartalena L, Bogazzi F, Braverman LE. The effects of amiodarone on the thyroid*. Endocr Rev. 2001;22:240–54. https://doi.org/10.1210/edrv.22.2.0427 .
Daniels GH. Amiodarone-induced thyrotoxicosis. J Clin Endocrinol Metab. 2001;86:3–8. https://doi.org/10.1210/JCEM.86.1.7119 .
Tanda ML, Piantanida E, Lai A, et al . Diagnosis and management of amiodarone-induced thyrotoxicosis: similarities and differences between North American and European thyroidologists. Clin Endocrinol (Oxf). 2008;69:812–8. https://doi.org/10.1111/j.1365-2265.2008.03268.x .
Article PubMed Google Scholar
Bartalena L, Wiersinga WM, Tanda ML, et al . Diagnosis and management of amiodarone-induced thyrotoxicosis in Europe: results of an international survey among members of the European Thyroid Association. Clin Endocrinol (Oxf). 2004;61:494–502. https://doi.org/10.1111/j.1365-2265.2004.02119.x .
Ataallah B, Buttar B, Kaell A, et al . Coronary vasospasm-induced myocardial infarction: an uncommon presentation of unrecognized hyperthyroidism. J Med Cases. 2020;11:140–1. https://doi.org/10.14740/jmc3473 .
Article PubMed PubMed Central Google Scholar
Choi YH, Jae HC, Sung WB, et al . Severe coronary artery spasm can be associated with hyperthyroidism. Coron Artery Dis. 2005;16:135–9. https://doi.org/10.1097/00019501-200505000-00001 .
Kuang XH, Zhang SY. Hyperthyroidism-associated coronary spasm: a case of non-ST segment elevation myocardial infarction with thyrotoxicosis. J Geriatr Cardiol. 2011;8:258–9. https://doi.org/10.3724/SP.J.1263.2011.00258 .
Malarkiewicz E, Dziamałek PA, Konsek SJ. Myocardial infarction as a first clinical manifestation of hyperthyroidism. Polish Ann Med. 2015;22:139–42. https://doi.org/10.1016/j.poamed.2015.03.007 .
Article Google Scholar
Pereira N, Parisi A, Dec GW, et al . Myocardial stunning in hyperthyroidism. Clin Cardiol. 2000;23:298–300. https://doi.org/10.1002/clc.4960230417 .
Gowda RM, Khan IA, Soodini G, et al . Acute myocardial infarction with normal coronary arteries associated with iatrogenic hyperthyroidism. Int J Cardiol. 2003;90:327–9.
Locker GJ, Kotzmann H, Frey B, et al . Factitious hyperthyroidism causing acute myocardial infarction. Thyroid. 1995;5:465–7. https://doi.org/10.1089/thy.1995.5.465 .
Homoncik M, Gessl A, Ferlitsch A, et al . Altered platelet plug formation in hyperthyroidism and hypothyroidism. J Clin Endocrinol Metab. 2007;92:3006–12. https://doi.org/10.1210/jc.2006-2644 .
Erem C. Blood coagulation, fibrinolytic activity and lipid profile in subclinical thyroid disease: subclinical hyperthyroidism increases plasma factor X activity. Clin Endocrinol (Oxf). 2006;64:323–9. https://doi.org/10.1111/j.1365-2265.2006.02464.x .
Dekkers OM, Horváth-Puhó E, Cannegieter SC, et al . Acute cardiovascular events and all-cause mortality in patients with hyperthyroidism: a population-based cohort study. Eur J Endocrinol. 2017;176:1–9. https://doi.org/10.1530/EJE-16-0576 .
Takasu N. Thyroid hormone and the cardiovascular system. Nippon rinsho. Japanese J Clin Med. 2006;64:2330–8.
Google Scholar
Kaderli RM, Fahrner R, Christ ER, et al . Total thyroidectomy for amiodarone-induced thyrotoxicosis in the hyperthyroid state. In: Experimental and clinical endocrinology and diabetes. Germany: Georg Thieme Verlag; 2015. p. 45–8.
Cappellani D, Papini P, Pingitore A, et al . Comparison between total thyroidectomy and medical therapy for amiodarone-induced thyrotoxicosis. J Clin Endocrinol Metab. 2020;105:242–51. https://doi.org/10.1210/clinem/dgz041 .
Cappellani D, Papini P, Di Certo agostino M, et al . Duration of exposure to thyrotoxicosis increases mortality of compromised AIT patients: the role of early thyroidectomy. J Clin Endocrinol Metab. 2020;105:E3427–36. https://doi.org/10.1210/clinem/dgaa464 .
Kotwal A, Clark J, Lyden M, et al . Thyroidectomy for amiodarone-induced thyrotoxicosis: Mayo Clinic experience. J Endocr Soc. 2018;2:1226–35. https://doi.org/10.1210/js.2018-00259 .
Quiroz-Aldave JE, Durand-Vásquez MC, Lobato-Jeri CJ, et al . Thyrotoxic cardiomyopathy: state of the art. Eur Endocrinol. 2023;19:78. https://doi.org/10.17925/ee.2023.19.1.78 .
Oe K, Yamagata T, Mori K. Acute myocardial infarction following hormone replacement in hypothyroidism. Int Heart J. 2007;48:107–11. https://doi.org/10.1536/ihj.48.107 .
Kassim TA, Clarke DD, Mai VQ, et al . Catecholamine-induced cardiomyopathy. Endocr Pract. 2008;14:1137–49.
Beyer C, Plank F, Friedrich G, et al . Effects of hyperthyroidism on coronary artery disease: a computed tomography angiography study. Can J Cardiol. 2017;33:1327–34. https://doi.org/10.1016/j.cjca.2017.07.002 .
Lin TH, Su HM, Voon WC, et al . Unstable angina with normal coronary angiography in hyperthyroidism: a case report. Kaohsiung J Med Sci. 2005;21:29–33. https://doi.org/10.1016/s1607-551x(09)70273-6 .
Bartalena L, Bogazzi F, Chiovato L, et al . 2018 European Thyroid Association (ETA) guidelines for the management of amiodarone-associated thyroid dysfunction. Eur Thyroid J. 2018;7:55–66.
Article CAS PubMed PubMed Central Google Scholar
Gough J, Gough IR. Total thyroidectomy for amiodarone-associated thyrotoxicosis in patients with severe cardiac disease. World J Surg. 2006;30:1957–61.
Tomisti L, Materazzi G, Bartalena L, et al . Total thyroidectomy in patients with amiodarone-induced thyrotoxicosis and severe left ventricular systolic dysfunction. J Clin Endocrinol Metab. 2012;97:3515–21. https://doi.org/10.1210/jc.2012-1797 .
Meerwein C, Vital D, Greutmann M, et al . Total thyroidectomy in patients with amiodarone-induced hyperthyroidism: when does the risk of conservative treatment exceed the risk of surgery? HNO. 2014;62:100–5.
Download references
Acknowledgements
Not applicable.
Author information
Authors and affiliations.
Clinic of Endocrinology, Diabetes and Metabolism, Hospital Delémont, Hôpital du Jura, Faubourg Des Capucins 30, 2800, Delémont, Switzerland
Yoann Aubry
Clinic of Endocrinology, Diabetes and Metabolism, University Hospital Basel, Basel, Switzerland
Yoann Aubry & Marc Y. Donath
The Division of Digestive Surgery, Surgery Department, University Hospitals of Geneva, Geneva, Switzerland
Michel Dosch
You can also search for this author in PubMed Google Scholar
Contributions
Yoann Aubry was involved in patient’s diagnosis and treatment plan. Yoann Aubry and Michel Dosch were involved in the literature research and writing. Marc Donath was supervising and correcting the work.
Corresponding author
Correspondence to Yoann Aubry .
Ethics declarations
Ethics approval and consent to participate, consent for publication.
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Competing interests
The authors declare that they have no competing interests. The content of the manuscript has not been published, or been submitted for publication elsewhere.
Additional information
Publisher's note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ . The Creative Commons Public Domain Dedication waiver ( http://creativecommons.org/publicdomain/zero/1.0/ ) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
Reprints and permissions
About this article
Cite this article.
Aubry, Y., Dosch, M. & Donath, M.Y. Cardiac evaluation in amiodarone-induced thyroid dysfunction with suspected cardiac ischemia?: a case report and review of the literature. J Med Case Reports 18 , 235 (2024). https://doi.org/10.1186/s13256-024-04552-w
Download citation
Received : 12 October 2023
Accepted : 08 April 2024
Published : 02 May 2024
DOI : https://doi.org/10.1186/s13256-024-04552-w
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Hyperthyroidism
- Cardiac ischemia
- Thyroidectomy
Journal of Medical Case Reports
ISSN: 1752-1947
- Submission enquiries: Access here and click Contact Us
- General enquiries: [email protected]
- Original research
- Open access
- Published: 29 April 2024
Development of a trigger tool to identify harmful incidents, no harm incidents, and near misses in prehospital emergency care
- Niclas Packendorff ORCID: orcid.org/0000-0002-0322-9471 1 , 2 ,
- Carl Magnusson 1 , 2 ,
- Kristoffer Wibring 3 , 4 ,
- Christer Axelsson 1 , 2 &
- Magnus Andersson Hagiwara 1
Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine volume 32 , Article number: 38 ( 2024 ) Cite this article
192 Accesses
1 Altmetric
Metrics details
Emergency Medical Services (EMS) are a unique setting because care for the chief complaint is given across all ages in a complex and high-risk environment that may pose a threat to patient safety. Traditionally, a reporting system is commonly used to raise awareness of adverse events (AEs); however, it could fail to detect an AE. Several methods are needed to evaluate patient safety in EMS. In this light, this study was conducted to (1) develop a national ambulance trigger tool (ATT) with a guide containing descriptions of triggers, examples of use, and categorization of near misses (NMs), no harm incidents (NHIs), and harmful incidents (HIs) and (2) use the ATT on randomly selected ambulance records.
The ambulance trigger tool was developed in a stepwise manner through (1) a literature review; (2) three sessions of structured group discussions with an expert panel having knowledge of emergency medical service, patient safety, and development of trigger tools; (3) a retrospective record review of 900 randomly selected journals with three review teams from different geographical locations; and (4) inter-rater reliability testing between reviewers.
From the literature review, 34 triggers were derived. After removing clinically irrelevant ones and combining others through three sessions of structured discussions, 19 remained. The most common triggers identified in the 900 randomly selected records were deviation from treatment guidelines (30.4%), the patient is non conveyed after EMS assessment (20.8%), and incomplete documentation (14.4%). The positive triggers were categorized as a near miss (40.9%), no harm (3.7%), and harmful incident (0.2%). Inter-rater reliability testing showed good agreement in both sessions.
This study shows that a trigger tool together with a retrospective record review can be used as a method to measure the frequency of harmful incidents, no harm incidents, and near misses in the EMS, thus complementing the traditional reporting system to realize increased patient safety.
Key messages
What is already known on this topic: The EMS system is potentially a high-risk environment for harmful incidents, and a reporting system could fail to detect adverse events; thus, new methods are needed.
What this study adds: This study adds an ATT to the clinical practice to complement the reporting system for the detection of harmful incidents, no harm incidents, and near misses and thus realize increased patient safety in EMS.
How this study might affect research, practice, or policy: The detection of harmful incidents, no harm incidents, and near misses in EMS could serve as a foundation for improving patient safety.
Over the recent decades, the Emergency Medical Services (EMS) system in Sweden has transitioned from a transport service to an emergency care service that provides advanced care and patient assessments at the scene, including triaging to the most optimal level of care [ 1 ]. EMS clinicians can manage common complaints of patients of all ages in a variety of settings. As they operate in high-risk environments that involve the occurrence of adverse events (AE) and threats to patient safety [ 2 ], methods are needed for evaluating patient safety.
Various methods have been developed to measure patient safety and AE frequency [ 3 ]. Reporting systems are one of the most common methods; however, they are effective only if medical staff are aware of the occurrence of an AE [ 4 , 5 ]. In EMS, a patient has few caregivers, and thus, the risk of an AE being missed is higher [ 6 ]. A structured retrospective record review (RRR) in combination with a trigger tool (TT) could complement a reporting system to detect up to 10 times more AEs [ 7 ]. Global Trigger Tool (GTT) is an example of a widely used tool of this type [ 8 ].
The report ‘To Err Is Human: Building a Safer Health System’ highlighted the need for working toward increased patient safety [ 9 ]. It was partly based on Harvard Medical Practice studies [ 9 , 10 , 11 ]. It revealed that 44,000–98,000 annual deaths at American hospitals were attributable to medical errors mainly due to drug complications, wound infections, and technical complications.
Few studies have investigated the incidence of AEs in EMS, although studies have adopted various methods. One explored the endotracheal intubation procedure performed by paramedics as it can easily be evaluated when arriving at the hospital; it found a fail rate of 25% [ 12 ]. Another study interviewed 15 EMS providers regarding events they recognized as an NM or AE; consequently, 50 events were categorized into errors prone to clinical judgement (54%), skill performance (21%), medications (15%), choice of destination (5%), and other (5%) [ 13 ].
One study conducted in Sweden used a TT originally developed in America for Helicopter Emergency Medicine Services (HEMS). It revealed a frequency of 4.3 AEs per 100 EMS missions [ 14 ]. The most common AE categorizes were unclear documentation and deviation from guidelines caused by mistakes made by the EMS clinicians. It also found higher AE incidence in patients with life-threating conditions.
To the best of our knowledge, no TT has been adapted for road-based EMS in western Europe. In this light, the present study aims to [ 1 ] develop a national ambulance trigger tool (ATT) with a guide containing descriptions of triggers, examples of use and categorization of near misses (NMs), no harm incidents (NHIs), and harmful incidents (HIs) and [ 2 ] use the ATT on randomly selected ambulance records.
The ATT was developed by a stepwise approach including the [ 1 ] review of existing literature regarding patient safety and areas of risk for AEs in the prehospital field [ 2 ] expert panel discussions with adaptation of the ATT through a video link, and [ 3 ] clinical evaluation of the ATT through RRR (Fig. 1 ).

Flow chart of the development process of the EMS trigger tool. EMS, emergency medical services. RRR, retrospective record review
The EMS system in Sweden is funded by taxes across regions, resulting in local variations in guidelines and documentation systems. At a national level, it was specified that in each ambulance, one of the two EMS clinicians must be a registered nurse (RN) often with a degree of master in ambulance/intensive/anaesthesiologic care.
We invited the majority of EMS organizations and three services were recruited across Sweden: an urban service with 85,000 EMS missions each year and a median mission time of 70 min and two urban–rural mixed services with 53,000 and 41,000 EMS missions each year and median mission times of 78 and 66 min, respectively. Two of these services participated in the first two sessions of structured discussions and the other one participated in the third.
Terminology and definitions
We used the World Health Organization (WHO) terminology for incidents including NM, NHI, and HI [ 15 , 16 ] and categorized the incidents according to the National Coordination Council for Medication Error Reporting and Prevention index (NCC MERP) [ 17 ].
An NM incident (e.g. lack of documentation) neither affects nor harms the patient but poses the risk of an error and is categorized as (A) or (B) according to the NCC MERP.
An NHI (e.g. omission of electrocardiogram (ECG) in patient with chest discomfort not diagnosed with acute coronary syndrome) affects the patient but does not cause harm. It is categorized as (C) ‘An incident that affected the patient but did not cause any harm’ or (D) ‘An incident that affected the patient and demanded observation or treatment to assure that no harm occurred’.
NMs and NHIs are traditionally not used when using TTs but could be valuable in terms of evaluating the clinical setting by receiving information about commonly occurring NMs and NHIs [ 18 ].
An HI (adverse event; e.g. omission of ECG in patient with chest discomfort and later diagnosed with ST-elevated myocardial infarction, thus delaying time to causal treatment) harms the patient. It is categorized as (E) ‘Contributed to or resulted in temporary harm and required intervention’; (F) ‘Contributed to or resulted in temporary harm requiring outpatient care, readmission, or prolonged hospital care’; (G) ‘Contributed to or caused permanent patient harm’; (H) ‘An event that required lifesaving intervention within 60 min’; or (I) ‘Contributed to the patient’s death’.
Step 1. Literature review
Existing TTs for inpatients, homecare, paediatric care, and psychiatric care presented by the Swedish Association of Local Authorities and Regions (SKR) were reviewed for developing the new ATT [ 19 ]. To cover a prehospital context and to identify risk areas for patient safety, PubMed, Cinahl and Medline was searched with the following keywords: patient safety, prehospital, ambulance, trigger tool, and adverse event. Headlines and abstracts were read and included with the following criteria (1) a description of incidents regarding patient safety in EMS measured with various methods, (2) ≥ 18 years of age, (3) not published before 1980.
Step 2. Expert panel and Structured discussions
Five experts, including RNs and medical doctors (MDs), were invited via email to contribute during the discussions. The RNs were eligible to participate in the development of the ATT if they had 10 years’ EMS clinical experience, previous experience in patient safety in an EMS organization, and experience regarding the usage of a TT. The MDs were recruited because of their knowledge and experience in the methodology of developing TTs. They were also responsible for patient safety in the healthcare system at a regional or national level within their organization. All members of the panel where confident in other methods used in the patient safety context such as incident reporting or root cause analysis. The experts were recruited on the authors opinions who was suitable but also depending on personal interest from the experts.
Three sessions of structured discussions was employed to reach a consensus among a panel of experts regarding the ATT, where the collective opinion of the group is deemed stronger than that of each individual [ 20 ]. An expert is known to be a specialist in their field, an individual who has knowledge on a specific matter [ 21 , 22 ]. During the three sessions, the discussions was structured as follows: each definition and trigger were analysed using a shared screen view for language, clinical relevance, and user-friendliness. The document was seen by all experts, and the removal, adaptation, or combination of triggers was done instantly. Each correction was approved by the experts before moving on to the next trigger. The session was video recorded so that the session would be viewable again and the corrections were emailed to the experts with the ability to give written feedback. Consensus was considered achieved when all experts had approved the ATT via email, and no further feedback was provided by them in writing.
Step 3. RRR process and Review teams
The measurement of patient safety with TTs requires access to patient records. In this light, review teams consisting of an RN and an MD were formed, where the RN starts with a primary review of the patient record with guidance of a list of triggers. A trigger can be a clue that an incident has occurred. Each trigger comes with a definition containing criteria that need to be fulfilled for the trigger to be considered positive.
The RN searches the records for positive triggers, reviews them for a potential incident, and classifies the incident according to the three first steps (AB, C, D) of the NCC MERP [ 17 ]. Records with an incident graded C and D undergo a secondary review by the MD, who assesses them for an HI. If an HI is found, the MD classifies it according to the last five steps (E, F, G, H, I) of the NCC MERP. The MD also classifies the type of HI and whether it is preventable by using the following scale: (1) ‘not preventable’; (2) ‘probably not preventable’; (3) ‘probably preventable’, and (4) ‘certainly preventable’.
The three EMS organizations each formed a review team consisting of a MD and a RN. The MD was in medical charge of their organization, and the RN had extensive experience of working in the EMS within this organization. One organization used two RNs having comparable experience in working in the EMS in the primary review.
In a pilot study before session two of the structured discussions, two review teams from two different organizations randomized 150 records and performed an RRR to gain experience in using the ATT.
Before session three of the structured discussions, three review teams from different organizations randomized 900 records and performed an RRR to further evaluate the ATT and to receive frequencies of positive triggers and incidents from their organizations. Before the RRR the review teams received training in how to extract and randomize data, how to use the ATT within Microsoft Access®, definitions of common terminology regarding a TT (e.g. positive trigger, NM, NHI, and HI), and examples with fictitious records. The reviewers had no previous experience in using a TT.
The criteria for inclusion in both RRR was age ≥ 18 years and a primary mission where a patient assessment takes place. Children were excluded in this study because several studies have shown that different triggers are required to study the paediatric population in EMS [ 23 , 24 ]. There are plans to develop a set of triggers adapted for children.
The positive triggers, NMs, NHIs, and HIs were presented in a frequency-based manner according to both the WHO and the NCC MERP. Each member of the review teams graded the triggers according to clinical relevance, comprehensibility, and utility with a 4-point Likert scale, where 1 = not relevant, 2 = somewhat relevant, 3 = quite relevant, and 4 = highly relevant after the RRR. The item-level content validity index (I-CVI) was calculated for each trigger by summing the number of reviewers grading trigger 3 or 4 and divided by the total number of reviewers. I-CVI of 0.80 or higher was considered highly relevant [ 25 ]. The positive predictive value (PPV) was calculated for each trigger by how many times the trigger resulted in a near miss, no harmful or harmful incident divided by the total times the trigger was found multiplied by 100 [ 26 ]. The Mersenne Twister algorithm was used for randomizing the records [ 27 ].
Two sessions of independent inter-rater reliability (IRR) tests between two primary reviewers were conducted, with the triggers serving as the variable for testing. The total outcome of positive triggers was summed up and analysed in a confusion matrix with Cohen’s kappa (Table 3 ) [ 28 ]. Kappa values of 0.21–0.40, 0.41–0.60, 0.61–0.80, and 0.81–1.00 were respectively considered fair, moderate, substantial, and almost perfect [ 29 ]. The ATT produces an overrepresentation of negative triggers when no incidents have occurred and creates a prevalence problem which causes Cohen’s kappa to be low [ 28 , 30 ]. Therefore, Cohen’s kappa was complemented with a prevalence-adjusted and bias-adjusted kappa (PABAK) [ 30 ]. The interpretation of PABAK and Cohen’s kappa is the same [ 31 ]. All analyses were performed with R studio version 2023.03.0 + 386.
Literature review
The review of previous TTs from SKR and the literature search using PubMed, Cinahl and Medline revealed 32 triggers (refer to supplement 1 and 2 ). The structure of the ATT was constructed to be the same as that of previous TTs from SKR, and each of the 32 triggers was defined and received definition for the trigger to be positive.
Structured discussion session one
The 32 triggers and definitions were emailed to the five experts two weeks before the planned session. After session one, a total of ten triggers were removed, reducing the number to 22. This was achieved by removing clinically irrelevant triggers or combining several triggers into one. These excluded triggers concerned areas that were either fully covered by other triggers after modifying their definition or were outside the scope of EMS. The majority of the removed triggers were related to EMS organizational quality aspects and were deemed beyond the scope of the EMS trigger review within the EMS record. Examples include triggers related to resource allocation, dispatch actions, or inactions (refer to supplement 2 ).
RRR with 150 records
To receive feedback from the clinical professionals regarding the 22 triggers, they were evaluated with RRR in clinical practice. Two EMS organizations formed review teams consisting of an RN as a primary reviewer and an MD as a secondary reviewer. The review teams were asked to use the ATT when reviewing randomized records from their organization. The aim of the review teams was to evaluate the clinical relevance, utility, and comprehensibility of the ATT in a clinical setting but also the usability of the digital database. The teams also documented time in minutes for each record reviewed. The ATT presented the following top three positive triggers from the 150 records, B1 Deviations from treatment guidelines in 47 (31%), A1 Incomplete documentation in 33 (22%) and B6 The patient is non conveyed after EMS assessment in 34 (22.7%). The review time was median 5 min per record with a range from 2 to 18 min. These experiences and result showed that the method was feasible, and the digital database was sufficient which served as a foundation for the next session of discussion.
Structured discussion session two
Session two consisted of members of the review teams from the RRR with 150 records. The review teams used their knowledge, experience, and result from the previously performed RRR to further adapt the definitions of the triggers. This round resulted in changes in trigger definitions; however, no trigger was removed or added for example A1 Incomplete documentation received five criteria to be considered positive and B5 Inconsistency between the EMS clinicians and emergency physicians assessment and triage received criteria to be positive if the patient were taken from the ED to definitive care (thrombolysis, percutaneous coronary intervention, intensive care) directly after the physicians assessment. (refer to supplement 2 ).
IRR session one based on 90 records
The first session of IRR testing between two primary reviewers was carried out on 90 records (Table 1 ). Cohen’s kappa k = 0.5 and PAPAK k = 0.89.
RRR with 900 records
The final use of the ATT consisted of three EMS organizations, where each organization formed review teams. The RNs categorized the records meeting the inclusion criteria by each month and randomized 25 per month in subject for review; 300 records per organization were used. Table 2 lists the demographics, and Table 3 lists the frequencies of positive triggers with PPV grouped by incidents, and Table 4 lists the classification of incidents according to the NCC MERP and WHO. Nine records were excluded from one mixed organization for not meeting the inclusion criteria. After the RRR, the members of the review teams received an online form consisting of the 4-point Likert scale in order to calculate I-CVI for each trigger presented in Table 5 .
IRR session two based on 90 records
In the second session of IRR testing, the same primary reviewers as those in the previous session conducted an RRR of the same 90 records, producing Cohen’s kappa k = 0.3 and PAPAK k = 0.88 (Table 1 ).
Structured discussion session three
In session three, both the experts and review teams (in total 12) were invited for a video meeting. Because of difficulties in gathering both the panel of experts and review teams, this round was divided into two groups with 10 participants. Two weeks before the session was scheduled, the experts and review team members received the frequencies from the previous RRR, including the I-CVI and IRR results. In this round, the number of triggers was reduced to 18 (refer to supplement 2 ), and the process of categorizing incidents was altered as follows. The primary examiner decided whether positive triggers in the patient records contributed to an incident, number of incidents, and whether the incident affected the patient with a risk of harm or not. Incidents that did not affect the patient or entail any risk of harm were classified according to the categories AB and C by the primary reviewer. An incident with a risk of the patient being harmed is secondary reviewed by a MD and no classification of the incident is made by the primary reviewer but left to the secondary reviewer. The secondary reviewer assessed incidents with a risk of harm and decided whether the patient was harmed or not. If the patient was not harmed, categories AB, C, and D were used. If the patient was harmed, the type of harm and degree of severity were assessed according to the categories E to I. Refer to supplement 3 for a translated manual of the final ATT.
Three structured discussion sessions were conducted with an expert panel, complemented by RRR, to develop the ATT. In this study, the sessions were held via video meetings, with trigger definitions displayed on a shared screen. The moderator made real-time changes to the document in consensus with the panel of experts. Several methods exist to achieve consensus among expert panels, with one of the most commonly used being the Delphi technique [ 32 ]. Anonymity is a key feature of conducting a Delphi survey, as it is argued to mitigate biases caused by hierarchy or individual dominance within the expert panel [ 33 ]. However, the technique has been modified in various ways, leading to questions regarding its methodology [ 34 , 35 ].
The original methodology employs a paper-based approach, where questionnaires are distributed to a panel of experts [ 20 ]. The researcher analyzes the responses to generate statements and questions, which are then rated by the experts in subsequent rounds [ 32 ]. The original Delphi has been suggested to be ineffective and error-prone [ 36 ].
The methodology used in this study has been successfully employed in previous studies for developing TTs [ 26 , 37 ]. We identify several advantages with this methodological approach compared to conducting a traditional Delphi survey. In Sweden, there is a limited number of experts regarding the use of trigger tools, especially within the context of EMS. While the size of a traditional Delphi panel can vary from 10 to 1000 [ 33 ], there is no standard number [ 38 ]. In this study, experts were selected based on personal invitations from the author using specific criteria (refer to the method section), which may impact the homogeneity of the group. A diverse group may lead to a broader discussion, whereas a homogeneous group may result in more reliable outcomes, depending on the study's aim [ 33 ]. However, including experts who are not knowledgeable about patient safety and the use of trigger tools in EMS could potentially negatively influence the identification of triggers by excluding those that may identify incidents. We believe that the panel size, complemented by literature review RRR in this study, was sufficient to develop a comprehensive TT covering most aspects of patient safety incidents in EMS.
The use of video meetings to conduct structured discussions was considered a strength as it allowed experts from various geographical locations to participate, thus enabling a higher degree of participation and reducing dropouts. While face-to-face discussions lacked anonymity, literature suggests that complete anonymity is challenging to achieve since the researcher knows the experts and there may be different relations between the experts not known by the researcher [ 34 ]. Due to the complexity of the triggers and definitions, we believe that there was an advantage in discussing the triggers face-to-face in a qualitative manner, rather than making them quantifiable using surveys. We utilized RRR as a quantitative component to gain clinical experience with the ATT to be used later in the structured discussions.
Face-to-face discussions are also utilized in other methodologies such as focus groups or the nominal group technique [ 39 , 40 ]. The lack of anonymity also appears to motivate experts to participate in the sessions [ 41 ]. Experts and review teams participating in the structured discussions were given the opportunity to provide written feedback individually after the meeting, allowing for corrections if issues regarding lack of anonymity were present during the discussions. Our experience from the current discussions is that no member dominated the discussion, and all were given the opportunity to express their opinion. The written feedback provided less input to the TT compared to the structured discussions.
The use of a TT comes with reliability issues between the reviewers, and studies have shown that even experienced review teams will review records differently [ 42 ]. The IRR also seems to decrease if the triggers are subjective [ 43 ]. To increase the IRR, it is recommended to use team training, a two-way review process, and reviews in consensus instead of independently [ 44 , 45 ]. This study used team training, a two-way review process, as well as a manual with definitions of the triggers to increase the IRR.
The most common triggers identified in the records were incomplete documentation, deviation from guidelines, and termination of patient care after the EMS clinician’s assessment. Incomplete documentation was found in 14% of patient records; although it might not contribute to an HI, it contributes substantially to NM, thus emerging as an important area for improvement in the EMS. One study [ 46 ] simulated the actions of EMS clinicians during medical or traumatic emergency care of a patient. The video-recorded actions were later compared with the documentation, and they revealed missing documentation in 22% of medical cases and 14% of traumatic cases. Incomplete documentation could be caused by several reasons; a study has shown that incomplete documentation poses a risk of errors when transferring a patient from the EMS to the emergency department (ED) because of differences in the verbal report and what is later recorded [ 47 ].
Deviation from guidelines was found in 30% of records and was further categorized as assessment/interventions according to SX-ABCDE (Scene safety, eXanguinating bleeding, Airway, Breathing, Circulation, Disability, Exposure), where (11%) of the deviations were found, along with absence of measured vital signs (8%), and absence of relevant clinical examination (16%). One record could have several positive triggers in the categorization of deviation from guidelines which affect patient care negatively. The assessment/interventions according to SX-ABCDE was positive if the EMS examiner failed to assess the scene safety or the patient’s XABCDE or failed to address issues according to the algorithm. The ABCDE approach is widely accepted by expert consensus in the medical, surgical, and anaesthetics field to improve the quality and speed of patient treatment [ 48 ].
The absence of measured vital signs was positive if the record failed to display the common vital signs, rate of breathing, saturation, blood pressure, pulse, and temperature. Blood-glucose was added if indicated for loss of consciousness or seizures. A study of non-conveyed patients showed vital signs data was missing in 6%–19% of patient records [ 49 ]. Studies have shown that both a lack of on-scene vital signs for trauma patients and a failure to notice deviations of vital signs at the ED were associated with increased mortality [ 50 , 51 , 52 ].
The absence of relevant clinical examination was positive if a patient did not receive appropriate examination in relation to the chief complaint. For example, if the patient’s chief complaint was chest pain and they were not examined with an ECG, or the chief complaint was abdominal pain but they did not receive an abdominal examination (e.g. auscultation, palpation). The prehospital ECG showed abnormalities in 19% of cases in comparison with the ECG at the ED, thus potentially affecting the prospective care of the patient [ 53 , 54 ].
The trigger ‘patient care is terminated after the ambulance nurse’s assessment’ was found in 20.8% of cases, and the trigger ‘patient contacted the ambulance or ED within 72 h for the same symptoms’ was found in 15.1% of cases, which correlates with previous findings [ 1 , 55 ].
The reviewers identified HI in two records (0.2%), NHI in 33 records (3.7%), and NM in 366 records (40.6%). A previous study [ 2 ] reported a frequency of 4.3% (46 out of 1080) in prehospital records using a different terminology with the AE potential for harm (43 out of 1080) and AE with harm identified (3 out of 1080). The different terminology used makes it difficult to make direct comparisons between the results of the studies; however, the HI in this study shows a similar result as AE with harm identified in the previous study.
Strengths and limitations
To our knowledge, this is the first study of EMS in which positive triggers are evaluated by a primary and secondary reviewer according to the NCC MERP [ 17 ]. This enables the categorization of the triggers into NMs, NHIs, and HIs according to the WHO, which could serve as a foundation for improvement within a given EMS organization [ 18 ].
One limitation in this study could be the number of participants of 12 which could affect the results in not recognizing possible areas of risk for patient safety in the prehospital environment. One limitation in reviewing records from the own organization thus creates a risk for underestimating the occurrence of positive triggers, NHs, NHIs, and HIs. Another limitation could be the failure to include a rural organization with a longer time of transport to participate. None of Sweden’s rural organizations agreed to participate in this study.
Conclusions
The EMS environment poses significant risks to patient safety, yet it remains inadequately studied. Conventional incident reporting systems often fall short in capturing these risks, necessitating a multifaceted approach to enhance patient safety. Our study introduces a tailored trigger tool for EMS, demonstrating its potential in identifying safety-threatening incidents. This tool provides a foundation for future research, offering a systematic means of incident detection and refinement. Beyond its immediate utility in incident detection within EMS, the trigger tool engenders a framework conducive to ongoing refinement and elucidation of trigger parameters and definitions, thus facilitating a deeper understanding of safety dynamics within the EMS.
Magnusson C, Herlitz J, Axelsson C. Patient characteristics, triage utilisation, level of care, and outcomes in an unselected adult patient population seen by the emergency medical services: a prospective observational study. BMC Emerg Med. 2020;20(1):7.
Article PubMed PubMed Central Google Scholar
Hagiwara MA, Magnusson C, Herlitz J, Seffel E, Axelsson C, Munters M, et al. Adverse events in prehospital emergency care: a trigger tool study. BMC Emerg Med. 2019;19(1):14.
Vincent C, Burnett S, Carthey J. The measurement and monitoring of safety. The Health Foundation. 2013. [cited 2021 May 4]. Available from: https://www.health.org.uk/publications/the-measurement-and-monitoring-of-safety .
Unbeck M, Muren O, Lillkrona U. Identification of adverse events at an orthopedics department in Sweden. Acta Orthop. 2008;79(3):396–403.
Article PubMed Google Scholar
Christiaans-Dingelhoff I, Smits M, Zwaan L, Lubberding S, van der Wal G, Wagner C. To what extent are adverse events found in patient records reported by patients and healthcare professionals via complaints, claims and incident reports? BMC Health Serv Res. 2011;11(1):49–59.
Meisel ZF, Hargarten S, Vernick J. Addressing Prehospital Patient Safety Using the Science of Injury Prevention and Control. Prehosp Emerg Care. 2008;12(4):411–6.
Classen DC, Resar R, Griffin F, Federico F, Frankel T, Kimmel N, et al. “Global trigger tool” shows that adverse events in hospitals may be ten times greater than previously measured. Health Aff. 2011;30(4):581–9.
Article Google Scholar
Griffin F, Resar R. IHI Global Trigger Tool for Measuring Adverse Events. 2009. Available from: http://app.ihi.org/webex/gtt/ihiglobaltriggertoolwhitepaper2009.pdf . [cited 2021 May 4]
Leape LL, Brennan TA, Laird N, Lawthers AG, Localio AR, Barnes BA, et al. The Nature of Adverse Events in Hospitalized Patients. N Engl J Med. 1991;324(6):377–84.
Article CAS PubMed Google Scholar
Brennan TA. Incidence of adverse events and negligence in hospitalized patients: results of the Harvard Medical Practice Study I. Qual Saf Health Care. 2004;13(2):145–51.
Article CAS PubMed PubMed Central Google Scholar
Localio AR, Lawthers AG, Brennan TA, Laird NM, Hebert LE, Peterson LM, et al. Relation between Malpractice Claims and Adverse Events Due to Negligence. N Engl J Med. 1991;325(4):245–51.
Katz SH, Falk JL. Misplaced endotracheal tubes by paramedics in an urban emergency medical services system. Ann Emerg Med. 2001;37(1):32–7.
Fairbanks RJ, Crittenden CN, O’Gara KG, Wilson MA, Pennington EC, Chin NP, et al. Emergency Medical Services Provider Perceptions of the Nature of Adverse Events and Near-misses in Out-of-hospital Care: An Ethnographic View. Acad Emerg Med. 2008;15(7):633–40.
World Health Organisation. Conceptual Framework for the International Classification for Patient Safety. 2009.
Google Scholar
Runciman W, Hibbert P, Thomson R, Van Der Schaaf T, Sherman H, Lewalle P. Towards an International Classification for Patient Safety: Key concepts and terms. Int J Qual Health Care. 2009;21(1):18–26.
National Coordinating Council for Medication Error Reporting and Prevention. NCC MERP Index for Categorizing Medication Errors. 2001.
Schildmeijer K, Unbeck M, Muren O, Perk J, Pukk Härenstam K, Nilsson L. Retrospective record review in proactive patient safety work - Identification of no-harm incidents. BMC Health Serv Res. 2013;13(1):282–9.
Swedish Association of Local Authorities and Regions (SKR). Marker based record review to identify and measure harm in health care. Stockholm: Swe: Markörbaserad Journalgranskning – för att identifiera och mäta skador i vården; 2012.
Hasson F, Keeney S, McKenna H. Research guidelines for the Delphi survey technique. J Adv Nurs. 2000;32(4):1008–15.
McKenna HP. The Delphi technique: a worthwhile research approach for nursing? J Adv Nurs. 1994;19(6):1221–5.
Goodman CM. The Delphi technique: a critique. J Adv Nurs. 1987;12(6):729–34.
Cottrell EK, O’Brien K, Curry M, Meckler GD, Engle PP, Jui J, et al. Understanding safety in prehospital emergency medical services for children. Prehosp Emerg Care. 2014;18(3):350–8.
Liu Y, Yan J, Xie Y, Bian Y. Establishment of a pediatric trigger tool based on Global Trigger Tool to identify adverse drug events of children: Experience in a Chinese hospital. BMC Pediatr. 2020;20(1):454–62.
Polit DF, Beck CT. The content validity index: Are you sure you know what’s being reported? Critique and recommendations Res Nurs Health. 2006;29(5):489–97.
Lindblad M, Schildmeijer K, Nilsson L, Ekstedt M, Unbeck M. Development of a trigger tool to identify adverse events and no-harm incidents that affect patients admitted to home healthcare. BMJ Qual Saf. 2018;27(7):502–11.
Matsumoto M, Nishimura T. Mersenne Twister: A 623-Dimensionally Equidistributed Uniform Pseudo-Random Number Generator. ACM Trans Model Comput Simul. 1998;8(1):3–30.
Cohen J. A coefficient of agreement for nominal scales. Educ Psychol Meas. 1960;20:37–46.
Landis JR, Koch GG. The Measurement of Observer Agreement for Categorical Data. 1977. Vol. 33, Source: Biometrics.
Book Google Scholar
Byrt T, Bishop J, Carlin JB. Bias, prevalence and kappa. J Clin Epidemiol. 1993;46(5):423–9.
Iftikhar S. Modification in inter-rater agreement statistics-a new approach. J Med Stat Inform. 2020;8(1):2.
Keeney S, Hasson F, McKenna HP. The Delphi technique in nursing and health research. Chichester, West Sussex: Wiley-Blackwell; 2011.
Nasa P, Jain R, Juneja D. Delphi methodology in healthcare research: How to decide its appropriateness. World J Methodol. 2021;11(4):116–29.
Keeney S, Hasson F, McKenna HP. A critical review of the Delphi technique as a research methodology for nursing. Int J Nurs Stud. 2001;38(2):195–200.
Boulkedid R, Abdoul H, Loustau M, Sibony O, Alberti C. Using and Reporting the Delphi Method for Selecting Healthcare Quality Indicators: A Systematic Review. PLoS ONE. 2011;6(6):e20476.
Deshpande AM, Shiffman RN, Nadkarni PM. Metadata-driven Delphi rating on the internet. Comput Methods Programs Biomed. 2005;77(1):49–56.
Unbeck M, Lindemalm S, Nydert P, Ygge BM, Nylén U, Berglund C, et al. Validation of triggers and development of a pediatric trigger tool to identify adverse events. BMC Health Serv Res. 2014;14(1):655–66.
Fink-Hafner D, Dagen T, Doušak M, Novak M, Hafner-Fink M. Delphi Method: Strengths and Weaknesses. Metodološki zvezki. 2019;16(2):1–19.
Kitzinger J. Qualitative Research: Introducing focus groups. BMJ. 1995;311(7000):299.
Foth T, Efstathiou N, Vanderspank-Wright B, Ufholz LA, Dü Tthorn EN, Zimansky M, et al. The use of Delphi and Nominal Group Technique in nursing education: A review. Int J Nurs Stud. 2016;60:112–20.
McKenna HP. The selection by ward managers of an appropriate nursing model for long-stay psychiatric patient care. J Adv Nurs. 1989;14(9):762–75.
Schildmeijer K, Nilsson L, Årestedt K, Perk J. Assessment of adverse events in medical care: lack of consistency between experienced teams using the global trigger tool. BMJ Qual Saf. 2012;21(4):307–14.
Naessens JM, O’Byrne TJ, Johnson MG, Vansuch MB, McGlone CM, Huddleston JM. Measuring hospital adverse events: assessing inter-rater reliability and trigger performance of the Global Trigger Tool. Int J Qual Health Care. 2010;22(4):266–74.
Forster AJ, Taljaard M, Bennett C, van Walraven C. Reliability of the Peer-Review Process for Adverse Event Rating. Morgan D, editor. PLoS One. 2012;7(7):e41239.
Classen DC, Lloyd RC, Provost L, Griffin FA, Resar R. Development and Evaluation of the Institute for Healthcare Improvement Global Trigger Tool. J Patient Saf. 2008;4(3):169–77.
Bergrath S, Rörtgen D, Skorning M, Fischermann H, Beckers SK, Mutscher C, et al. Notärztliche Einsatzdokumentation in der Simulation : Videobasierte Fehleranalyse. Anaesthesist. 2011;60(3):221–9.
Lubin JS, Shah A. An Incomplete Medical Record: Transfer of Care From Emergency Medical Services to the Emergency Department. Cureus. 2022;14(2):1–5.
Thim T, Krarup, Grove, Rohde, Lofgren. Initial assessment and treatment with the Airway, Breathing, Circulation, Disability, Exposure (ABCDE) approach. Int J Gen Med. 2012;5(1):117–21.
Höglund E, Andersson-Hagiwara M, Schröder A, Möller M, Ohlsson-Nevo E. Characteristics of non-conveyed patients in emergency medical services (EMS): a one-year prospective descriptive and comparative study in a region of Sweden. BMC Emerg Med. 2020;20(1):61.
Laudermilch DJ, Schiff MA, Nathens AB, Rosengart MR. Lack of Emergency Medical Services Documentation Is Associated with Poor Patient Outcomes: A Validation of Audit Filters for Prehospital Trauma Care. J Am Coll Surg. 2010;210(2):220–7.
Ljunggren M, Castrén M, Nordberg M, Kurland L. The association between vital signs and mortality in a retrospective cohort study of an unselected emergency department population. Scand J Trauma Resusc Emerg Med. 2016;24(1):21–31.
Brekke IJ, Puntervoll LH, Pedersen PB, Kellett J, Brabrand M. The value of vital sign trends in predicting and monitoring clinical deterioration: a systematic review. Patman S, editor. PLoS One. 2019;14(1):e0210875.
Davis MT, Dukelow A, McLeod S, Rodriguez S, Lewell M. The utility of the prehospital electrocardiogram. CJEM. 2011;13(06):372–7.
Davis M, Lewell M, McLeod S, Dukelow A. A Prospective Evaluation of the Utility of the Prehospital 12-lead Electrocardiogram to Change Patient Management in the Emergency Department. Prehosp Emerg Care. 2014;18(1):9–14.
Höglund E, Schröder A, Andersson-Hagiwara M, Möller M, Ohlsson-Nevo E. Outcomes in patients not conveyed by emergency medical services (EMS): a one-year prospective study. Scand J Trauma Resusc Emerg Med. 2022;30(1):1–10.
Download references
Open access funding provided by University of Boras. Sveriges Kommuner och Regioner (SKR)
Author information
Authors and affiliations.
Prehospen–Centre for Prehospital Research, Faculty of Caring Science, Work Life and Social Welfare, University of Borås, Borås, Sweden
Niclas Packendorff, Carl Magnusson, Christer Axelsson & Magnus Andersson Hagiwara
Department of Prehospital Emergency Care, Sahlgrenska University Hospital, Gothenburg, Sweden
Niclas Packendorff, Carl Magnusson & Christer Axelsson
Department of Ambulance and Prehospital Care, Region Halland, Sweden
Kristoffer Wibring
Institute of Health and Care Sciences, Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden
You can also search for this author in PubMed Google Scholar
Contributions
MH planned the study and developed the research design. NP, CM, planned, created the software/database. NP and KW carried out the data collection. NP wrote the first draft. All authors actively contributed to the final version of the manuscript. All authors read and approved the final version.
Corresponding author
Correspondence to Niclas Packendorff .
Ethics declarations
Competing interests.
The authors declare that they have no competing interests.
Additional information
Publisher’s note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Supplementary material 1., supplementary material 2., supplementary material 3., rights and permissions.
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ . The Creative Commons Public Domain Dedication waiver ( http://creativecommons.org/publicdomain/zero/1.0/ ) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
Reprints and permissions
About this article
Cite this article.
Packendorff, N., Magnusson, C., Wibring, K. et al. Development of a trigger tool to identify harmful incidents, no harm incidents, and near misses in prehospital emergency care. Scand J Trauma Resusc Emerg Med 32 , 38 (2024). https://doi.org/10.1186/s13049-024-01209-x
Download citation
Received : 26 June 2023
Accepted : 21 April 2024
Published : 29 April 2024
DOI : https://doi.org/10.1186/s13049-024-01209-x
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine
ISSN: 1757-7241
- Submission enquiries: Access here and click Contact Us
- General enquiries: [email protected]
- Open access
- Published: 29 April 2024
Untangling the mess of CGRP levels as a migraine biomarker: an in-depth literature review and analysis of our experimental experience
- Gabriel Gárate 1 ,
- Julio Pascual 1 ,
- Marta Pascual-Mato 1 ,
- Jorge Madera 1 ,
- María Muñoz-San Martín 1 &
- Vicente González-Quintanilla 1
The Journal of Headache and Pain volume 25 , Article number: 69 ( 2024 ) Cite this article
472 Accesses
9 Altmetric
Metrics details
Calcitonin gene-related peptide (CGRP) is the most promising candidate to become the first migraine biomarker. However, literature shows clashing results and suggests a methodological source for such discrepancies. We aimed to investigate some of these methodological factors to evaluate the actual role of CGRP as biomarker.
Previous to the experimental part, we performed a literature review of articles measuring CGRP in migraine patients. Using our 399 bio-bank sera samples, we performed a series of experiments to test the validity of different ELISA kits employed, time of sample processing, long-term storage, sampling in rest or after moderate exercise. Analysis of in-house data was performed to analyse average levels of the peptide and the effect of sex and age.
Literature review shows the high variability in terms of study design, determination methods, results and conclusions obtained by studies including CGRP determinations in migraine patients. CGRP measurements depends on the method and specific kit employed, also on the isoform detected, showing completely different ranges of concentrations. Alpha-CGRP and beta-CGRP had median with IQR levels of 37.5 (28.2–54.4) and 4.6 (2.4–6.4)pg/mL, respectively. CGRP content is preserved in serum within the 24 first hours when samples are stored at 4°C after clotting and immediate centrifugation. Storages at -80°C of more than 6 months result in a decrease in CGRP levels. Moderate exercise prior to blood extraction does not modulate the concentration of the peptide. Age positively correlates with beta-CGRP content and men have higher alpha-CGRP levels than women.
Conclusions
We present valuable information for CGRP measurements in serum. ELISA kit suitability should be tested prior to the experiments. Alpha and beta-CGRP levels should be analysed separately as they can show different behaviours even within the same condition. Samples can be processed in a 24-h window if they have been kept in 4°C and should not be stored for more than 6 months at -80°C before assayed. Patients do not need to rest before the blood extraction unless they have performed a high-endurance exercise. For comparative studies, sex and age should be accounted for as these parameters can impact CGRP concentrations.
Graphical Abstract
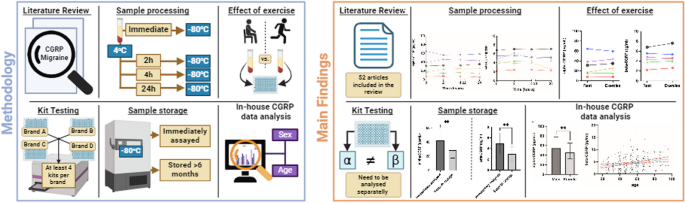
Peer Review reports
Introduction
Migraine and its subtypes are diagnosed based on clinical criteria [ 1 ]. Thus, multiple phenotypes sharing the same diagnosis are treated the same way with clashing outcomes. However, as many real-world data studies have shown [ 2 ], the different phenotypes have been proved ineffective to create profiles prone to respond to the different treatment options. Historical therapies for migraine, which is worth to mention that none of these were initially developed to treat this condition, apart from the triptans, and are not specific for it [ 3 ], have not met the challenge of effectively aborting and/or preventing the symptoms, in some cases with limited efficacy, tolerability and patient adherence [ 4 ].
Since the 1990s decade our understanding of migraine has expanded markedly and new therapeutic agents have been brought to the market in an effort to alleviate the personal and economic burden that migraineurs suffer. These are the calcitonin gene-related peptide (CGRP)-targeted therapies which have revolutionized the management of migraine [ 5 ], including monoclonal antibodies against the CGRP ligand or its receptor [ 6 ], and small molecules antagonists to the CGRP receptor, the gepants [ 7 ]. Nonetheless, there is still a portion of patients who do not respond to the treatments, highlighting the importance that a biomarker would have in migraine, allowing to create objective diagnostic criteria besides the clinical ones, which may be subject to errors [ 8 ], and to monitor objectively the response to treatments.
CGRP is a multifunctional neuropeptide which was first discovered in 1982, described as the result of the alternative splicing of the calcitonin gene (CALCA in humans) transcript, hence its name [ 9 ]. Later on, this first form of CGRP will be named alpha-CGRP, as opposed to the beta-CGRP, encoded in a different gene (CALCB in humans), with a different regulation and expression pattern to the alpha-CGRP [ 10 ]. These two peptides differ in 3 out of the 37 amino acids of their sequence but share a common structure and are part of the CGRP peptide family, also comprised by calcitonin, adrenomedullin 1 and adrenomedullin 2 [ 11 ]. Although their distribution in the human body tends to overlap [ 12 ], alpha-CGRP has been described to be the predominant form in the central and peripheral nervous system while beta-CGRP is more relatively abundant in the enteric nervous system [ 13 ].
The relevance of the peptide goes beyond its use as a therapeutical target, having been proposed as a biomarker in migraine. Several studies have reported elevation of the peptide in ictal and/or interictal phases in medication-free periods of migraine patients [ 14 , 15 , 16 , 17 , 18 , 19 , 20 , 21 , 22 , 23 , 24 , 25 , 26 , 27 , 28 , 29 , 30 , 31 , 32 , 33 , 34 , 35 , 36 , 37 , 38 ], the reduction of the CGRP levels after abortive and prophylactic treatment [ 26 , 28 , 38 , 39 , 40 , 41 , 42 , 43 , 44 ] and the induction of migraine-like headaches when infused in humans [ 45 ]. Despite these results, there are other works contradicting the findings [ 35 , 46 , 47 , 48 , 49 , 50 , 51 , 52 , 53 , 54 ] and which emphasize the way until its eventual validation and clinical use is still far way to become a reality. The source of such discrepancies, although still unknown, is most probably multifactorial. There is a methodological component [ 55 , 56 ] and the influence of other individual parameters such as comorbidities [ 36 ], concomitant treatments [ 57 ] or menstrual cycle [ 58 , 59 ], which have not been taken into account or which have not been sufficiently described to be considered properly.
In this work we have analysed in detail the existing literature about CGRP measurements in migraine patients, discussing their methodological differences and their effect on the reported concentrations of the peptide. In addition, we have conducted a series of experiments aimed to elucidate the potential effects on serum content of total CGRP, alpha-CGRP, and beta-CGRP, of a number of variables, including different enzyme-linked immunosorbent assay (ELISA) kits, sample processing time, long-term storage or immediate practise of exercise before sampling. Finally, we have analysed our in-house database of CGRP measurements to investigate the effect that sex and age might have on the molecules.
Review of previously published works including CGRP measurements in migraine patients
A systematic search was conducted in the databases PubMed, Scopus and Science Direct until February 2024 using the following terms: (a) CGRP; (b) migraine; and one of the following terms: (c) levels; (d) concentration; (e) measurements. We included original articles with CGRP measurements in humans with migraine. We only included and analysed works written in English language.
Methodological experiments
Kit analysis.
We tested 4 different ELISA kit references with serum samples, 2 based on competitive ELISA (Biorbyt, UK, ref: orb438605; BMA Biomedicals, Switzerland, ref: S-1198), specifically designed for the detection of total-CGRP, and 2 based on ELISA sandwich (Abbexa, UK, ref: abx257902; CUSABIO, China, ref: CSB-E08210h), designed for the detection of alpha and beta-CGRP, respectively. All 4 of these products were assayed multiple times (at least 4 for each kit reference) to analyse the optimal dilutions of the samples, their reproducibility and their reported concentrations. All the procedures were carried out strictly following the manufacturer’s instructions of use of their products, they were performed by the same researcher, using the same equipment, and in the same facilities. Regarding the last step of the ELISA processes, in which manufacturers give a window of time, specifying that the user must determine the optimum, we incubated the substrate for 15 min for alpha-CGRP and for 20 min for beta-CGRP. All the samples were measured in duplicate, obtained from morning blood extractions, 9–12 am, from patients in a fast of at least 12h. These samples were let to clot for 10–15 min, centrifuged at 3500 rpm for 10 min and then immediately stored at -80°C until assayed. A standard curve was generated for every single batch, and they were calculated using a 4-parameter logistic (4-PL) regression with r 2 > 0.999.
Influence of sample processing time
We recruited 6 individuals without history of migraine and subjective absence of headache at the day of the sampling (50% male; age range: 24–65 years). These individuals had a blood extraction in the early morning, between 9 am and 9:30 am, performed in rest at our laboratory facilities. The blood was then let to clot for 10 min at room temperature, then centrifuged at 3500 rpm for 10 min to obtain serum. Serum was divided into 4 tubes. First one was immediately stored at -80°C, the other three were kept in the refrigerator at 4°C for, 2, 4 and 24 h respectively before frozen. None of the samples were added peptidase inhibitor. These samples were measured by triplicate.
Effect of exercise
Additionally, after the first blood extraction, these same 6 subjects were asked to perform a 20 min run at moderate pace before a second blood extraction. Blood obtained was then processed following the same procedure as the resting samples but in this case all the serum was immediately stored at -80°C. These samples were measured by triplicate.
Long-term storage
We assayed 11 consecutive samples from previous works (36.4% male; age range: 26–65) that had been stored at -80°C for more than 6 months and which had been assayed altogether before being stored for a month and before reaching this time point.
Analysis of our CGRP database
Samples coming from our bio-bank were grouped together, reaching 399 individuals (29.3% male; age range: 18–96 years), and then analysed to see the average levels of the peptide and possible effects of sex and age in the circulating concentrations of the molecules.
Statistical analysis
Data are displayed as average with standard deviation (SD) unless stated differently. Comparisons between samples immediately processed and stored at -80°C obtained in resting subjects and right after exercising, and samples analysed before and after they had been stored for 6 months were made using the Wilcoxon matched-pairs signed rank test. Comparisons between samples from same individuals that were frozen at different timepoints have been made using Friedman test followed by Dunn’s test. Correlation relationships of the meta-analysis were evaluated by Spearman correlation test and summarized by Spearman’s rho coefficient and related p-values. Comparisons between sub-groups in the meta-analysis were performed using the Mann Whitney U test.
Article review
Applying the criteria specified in the method section we included 52 articles from the initial search that have been sorted by sample source and detection methodology and are displayed in Table 1 .
Out of these 52 articles, the main source of sample were blood extractions, with 44 (84.6%) works performing them. Twenty-eight (53.8%) used plasma samples, 6 (11.5%) from the jugular vein and the remaining 22 (42.3%) from the cubital vein. Serum was employed in 16 (30.8%) of the studies. Continue by order of use, saliva was the third sample source with 7 (13.5%), followed by cerebrospinal fluid (CSF) with 3 (5.8%) and by tear fluid with 2 (3.8%), and last, gingival crevicular fluid (GCF) with 1 (1.9%). According to the determination method, 21 (40.4%) of the studies measured CGRP by radioimmunoassay (RIA), 2 (3.8%) of them together with Bradford protein assay (Bradford), and 29 (55.8%) by ELISA, 1 (1.9%) performed along with bicinchoninic acid protein assay (BCA), and 2 (3.8%) used undefined enzyme immune assay (EIA).
Seventeen (32.7%) studies did not include healthy controls while the remaining 35 (67.3%) did. Sampling of the migraine patients were performed only in the ictal phase for 5 (9.6%) studies, only in the interictal phase for 20 (38.5%), in both phases for 22 (42.3%) works, and in 5 (9.6%) of them the phase was not specified.
Data was presented in different ways including mean ± standard deviation, ± standard error of mean (SEM), ± 2*SEM; median with range, interquartile range (IQR), 95% confidence intervals (CI), and in multiple units, pmol/L, fmol/mL, pmol/mg of total protein, pg/mL, pg/µg of total protein.
Therefore, these methodologies, sampling differences and variable data displays did not allow for a meta-analysis, and the absolute CGRP range among all the studies could be inferred, showing a wide range of concentrations (2.45–219,700 pg/mL) [ 28 , 54 ].
Experimental results
The kit from Biorbyt showed an elevated content of CGRP (range: 150-980pg/mL) compared to what has been reported in the bibliography [ 24 , 25 , 26 , 27 , 29 , 38 , 49 , 54 ] when undiluted serum samples were used. Moreover, the reproducibility of the kit was not satisfactory as the assayed samples did not meet the intra and inter-assay coefficient of variance criteria set by the manufacturer (> 10% and > 12%, respectively). This kit also showed a total lack of linearity for the dilutions of 1:2, 1:4, 1:8, 1:16 and 1:32 with each dilution showing higher CGRP concentrations than the one before (data not shown).
For BMA Biomedical kit we were unable to obtain a single measurement within the detection range. Since we decided to strictly follow the manufacturer’s instructions, we could not modify the standard curve points. All the readout absorbance measurements from the tested samples exceed the absorbance range obtained from the readout of the standard curve, and because this is a competitive ELISA technique, no dilution could be tested and neither we could assayed the reproducibility of the test.
Alpha-CGRP specific kit, from Abbexa, showed similar CGRP concentrations (range: 25-105pg/mL) to what has been described previously in most studies using serum from our group [ 38 , 69 , 70 ] and others [ 25 , 26 , 27 , 49 ]. Most of the samples fall within mid-range of the standard curve but the kit showed a good linearity of the measurements when samples were diluted 1:2, 1:3, 1:4 and 1:8 (data not shown). Across the different plates results fulfilled the reproducibility criteria by having an intra and inter-assay coefficient of variance below the maximum set by the manufacturer (< 8% and < 10%, respectively).
The last kit, from CUSABIO, showed similar beta-CGRP concentrations than reported in the literature (range: 1.6–10.5pg/mL) [ 31 , 35 , 36 , 38 , 70 , 71 ]. Because the samples fall within the lower part of the standard curve dilution of 1:2, 1:3 and 1:4 resulted in a lack of signal and the impossibility to determine the concentration of the peptide in all the samples but those with the higher beta-CGRP content. In this latter group the linearity found was between the ranges supplied by the manufacturer. Across the different plates results fulfilled the reproducibility criteria by having an intra and inter-assay coefficient of variance below the maximum set by the manufacturer (< 8% and < 10%, respectively).
Because the 2 kits based on competitive ELISA did not meet the quality requirements and did not adjust to the reported units in the literature the following experiments were carried out using the kits from Abbexa and CUSABIO which have been used by our group in previous studies [ 38 , 69 , 70 , 71 ].
We did not find changes in alpha nor beta-CGRP across samples which remained for 2 h (alpha: 29.9 ± 18.6pg/mL; beta: 4.9 ± 1.7pg/mL), 4 h (alpha: 30.4 ± 18.2pg/mL; beta: 4.7 ± 1.5pg/mL) and 24 h (alpha: 30.2 ± 19.6pg/mL; beta: 4.4 ± 1.8pg/mL) at 4°C compared to those which got deep frozen right away (alpha: 29.2 ± 20.6pg/mL; beta: 4.6 ± 1.6pg/mL; p = 0.99; p = 0.84; p = 0.99; respectively) (Fig. 1 ).

Sample processing: evolution of individual A alpha-CGRP and B beta-CGRP values for each subject throughout the time samples remained stored at 4°C before froze at -80°C
No differences were found in none of the molecules when comparing serum samples obtained in rest an immediately stored at -80°C and those obtained after exercise and with the same processing protocol (alpha: 31.1 ± 19.0pg/mL; beta: 4.8 ± 1.7pg/mL; p = 0.44) (Fig. 2 ).

Effect of exercise: evolution of individual A alpha-CGRP and B beta-CGRP values for each subject when sampling was performed in rest of after 20 minutes of moderate exercise
The first significant differences between samples which were measured before they remained stored at -80°C for a month (alpha: 42.3 ± 15.1pg/mL; beta: 4.9 ± 2.0pg/mL) and assayed after this date appeared from the sixth month of storage for both alpha-CGRP and beta-CGRP (alpha: 28.6 ± 11.3pg/mL, p < 0.01; beta: 3.0 ± 1.3pg/mL, p < 0.01) (Fig. 3 ).

Effect of storage: changes of individual A alpha-CGRP and B beta-CGRP values when samples were immediately analysed or analysed when they surpassed 6 months storage. Data is shown as average ± SD. Comparisons were made using Wilcoxon matched-pairs signed rank test. ** p < 0.01
Analysis of our database
Alpha and beta-CGRP did follow a normal distribution and averaged (median with IQR) 37.5 (28.2–54.4)pg/mL and 4.6 (2.4–6.4)pg/mL, respectively. Spearman correlation between alpha-CGRP and age was non-significant ( p = 0.300; r = -0.05), while it was significant for beta-CGRP and age ( p < 0.0001; r = 0.24). When these correlations were analysed with females and males alone it kept being non-significant for alpha-CGRP (male: p = 0.151, r = -0.14; female: p = 0.514, r = -0.04) and significant for beta-CGRP (male: p = 0.028, r = 0.21; female: p < 0.0001, r = 0.26). Alpha and beta-CGRP levels did not correlate significantly ( p = 0.056; r = 0.11). When sorted by sex, groups had no significant differences in their age distribution (male: 55.6 ± 17.7 years; female: 54.1 ± 16.9 years; p = 0.222), and showed significant differences in their alpha-CGRP content (median [IQR]; males: 54.4 [38.1–77.6] pg/mL; females: 45.2 [32.5–65.3] pg/mL; p < 0.01) and unaltered beta-CGRP levels (median [IQR]; males: 4.0 [2.3–6.2] pg/mL; females: 3.9 [2.1–6.1] pg/mL; p = 0.728) (Fig. 4 ).

In-house data analysis: A distribution of alpha-CGRP levels vs. age, green line represents a linear regression and red dotted line represents the CI; B distribution of beta-CGRP levels vs. age, green line represents a linear regression and red dotted line represents the CI; C distribution of beta-CGRP vs. alpha-CGRP levels, green line represents a linear regression and red dotted line represents the CI; D comparison of alpha-CGRP concentrations in subjects sorted by sex; E comparison of alpha-CGRP concentrations in subjects sorted by sex. Data is shown as average ± SD. Comparisons were made using Mann–Whitney U test, ns: non-significant; ** p < 0.01
Our literature analysis (Table 1 ) shows that studies based on CGRP determinations are highly variable in terms of measuring method and study design, including sample source, sample processing, inclusion/exclusion criteria for patients and controls and aim of the study [ 14 , 15 , 19 , 31 , 39 , 42 , 60 , 66 , 68 ]. Data analysis and presentation of laboratory determinations is also changeful, which hinder the comparison of the data. Despite all the difficulties, it results obvious that the overall outcomes and the conclusions drawn from them are inconsistent across works. Some authors have hypothesized that methodological differences might be the reason for such discrepancies [ 55 , 56 ], and, although this is likely to be the case, there is not to date a consensus of how CGRP determinations should be carried out.
If we analyse the methods used to measure CGRP in migraine patients we can see there have been mainly based on two different techniques, RIA and ELISA. RIA was the first, and until the late 2000s, the only one employed. RIA is based on the competitive incubation for specific antibody sites to form antigen–antibody complexes of radio-labelled and native unlabelled antigen. At equilibrium, the complexes formed are separated from the unbound antigen with a resulting ratio between these two. The bound/free antigen ratio is dependent on the amount of native antigen present in the sample as the radio-labelled is always added at a stable known concentration [ 72 ]. Therefore, this technique relies on the antiserum used, which has to provide an appropriate specificity in order to detect the antigen but no other analogues, and a proper affinity to do so in the range of interest.
The use of different antisera across all the CGRP-measuring studies based on RIA is a main source of variability among articles (Table 1 ). Works employing the same protocol, antiserum, and sample source usually have similar peptide concentrations [ 14 , 39 , 47 ], with some exceptions [ 48 ], while the use of different brands containing different antiseras and protocols show differing concentration ranges even when performed with same sample source [ 15 , 39 , 63 , 64 ], and even if they were done by the same specialist technician with the same samples [ 48 ]. Another problem is that even though studies with the exact same quantification method obtain similar concentration ranges they arrive to clashing conclusions, such as the presence of differences in CGRP concentrations between interictal migraine patients and healthy controls [ 17 , 65 ].
ELISA technique first appears to be used to determine CGRP concentration in migraine patients in 2007 [ 21 ]. ELISA is an immunological assay based on the interaction between the antigen and a primary antibody against the antigen of interest. These will interact, forming a complex that is later confirmed through the enzyme-linked antibody catalysis of an added substrate, which can be quantitatively measured using readouts from either a luminometer or a spectrophotometer. ELISA techniques are broadly classified into direct, indirect, sandwich, and competitive ELISA. For CGRP determinations only competitive and sandwich ELISA have been employed. Competitive ELISA involves a competition between the sample antigen and the plate-coated antigen for the primary antibody, followed by the binding of enzyme-linked secondary antibodies (Fig. 5 ). Sandwich ELISA technique includes a sample antigen introduced to the antibody-precoated plate, followed by sequential binding of detection and enzyme-linked secondary antibodies to the recognition sites on the antigen (Fig. 6 ) [ 73 ]. In both cases, and similarly to what has been pointed out for RIA, the techniques rely on the specificity and sensitivity of the antibodies included in the kit. This is the reason why ELISA-based studies are also subjected to the exact same issues associated with RIA-based works. As it has been described, investigations using the same brand also reports similar peptide concentration ranges [ 25 , 26 , 30 , 44 , 49 , 67 ], even though this is not always the case [ 32 ], but, most importantly, those using different kits clash in the range of concentrations [ 23 , 61 , 62 ] on top of the conclusions drawn [ 33 , 61 ]. For this point we need to explain that kits from USCN Life Sciences and Cloud Clone Corp., and from Peninsula Laboratories and BMA Biomedicals have been considered as only two brands since these companies have merged or have been acquired by the other at some point in their history. Moreover, and this last point serves as an example, there is a lack of information by part of the researchers regarding the kits used, because sometimes the brand cited offers more than one kit or two different brands over the history have been in charge of its production, and with the given information it cannot be inferred which one it was [ 27 , 34 ]. This could be the reason why across studies using kits from the same brand they obtained different concentrations. Also, this lack often comes from the manufacturers, which most of the times do not report essential information to the user such as the specific epitope recognised by the antibodies or their cross-reactivity for analogues of CGRP. This has caused some controversies such as works employing kits specifically designed, according to the manufacturer, for the detection of beta-CGRP reporting results as total-CGRP [ 35 , 36 , 59 ] without proving in their papers whether the technique recognises alpha, beta, or total-CGRP.

Schematic representation of a competitive ELISA protocol

Schematic representation of a sandwich ELISA protocol
CGRP has been analysed in a broad number of samples sources including plasma and serum from the peripheral circulation and jugular vein, CSF, saliva, tear fluid and GCF. Due to the enormous variability of concentrations found within the sources (Table 1 ) and the fact that results are not homogenous even when the same technique and sample source were used, we thought the comparison between sample sources did not make sense.
Nonetheless, and because our group has focused on the determinations in serum with ELISA, we have done a specific analysis of the studies matching these two criteria. There seems to be a consensus range achieved by most of the studies, independently of the brand employed, and which approximately goes from 15 to 150 pg/mL for total and alpha-CGRP, because the data from the literature exhibits that most of the measured CGRP is the alpha isoform, and from 2 to 10 pg/mL for beta-CGRP.
Because there are examples of different works employing the same method, specific technique, sample source and similar inclusion/exclusion criteria whose results are contradictory [ 14 , 33 , 47 , 59 ], we cannot conclude that all the problematic with CGRP measurements is related to the quantifying method and/or the sample chose by the authors. There has to be other factors playing a role in the discrepancies, such as fluctuations with the circadian [ 74 ] or with the menstrual cycles [ 58 , 59 , 75 ], effect of resting/exercise [ 76 , 77 ], fast degradation of the peptide due to its short half-life [ 78 ], long-term storage stability [ 55 ], migraine and other comorbidities [ 69 , 71 , 79 , 80 , 81 ], and the effects of pharmacological treatments [ 26 , 28 , 38 , 39 , 40 , 41 , 42 , 43 , 44 ]. From our review we could not analyse these parameters, because they were not displayed with enough accuracy in most articles.
Experimental studies
Here, in an effort to provide more detailed information about the suitability of serum from peripheral blood for CGRP determinations, we carried out a series of experiments in order to shed light on some of the main questions regarding the lack of consistency with CGRP quantifications beyond the data already discussed from our review.
We have found that the specific ELISA kit employed has a crucial effect on the CGRP measurements, showing completely different concentration ranges depending on the reference.
Besides the differences in the range we have obtained some alarming results. One of the kits assayed, from Biorbyt, did not meet the reproducibility criteria, which automatically should make this kit unsuitable for any kind of research. On top of that it did not conserve the linearity when diluting the samples which adds more doubts to its reliability. The one from BMA Biomedicals, even though a kit from this brand has been used for a published work when the company had the name Peninsula Laboratories [ 24 ], showed for 4 different times results below the detection limit (20pg/mL), contradicting the data of the cited article. Once again, these data call for a more exhaustive description of the methodology, not only by the researchers but also the companies.
The other two kits assayed fulfilled all the quality requirements and presented a range of measurements which fit the range observed in studies using the same sample source. Because the kit from CUSABIO is specific for beta-CGRP we have considered that the objective range for this kind of determination is different to the range for the Abbexa kit, which detects alpha-CGRP. This comes with no surprise because notwithstanding we have not displayed it, in our previous works the exact internal validations were performed and our researches already shown that these kits were reliable and were in accordance with the results published in the past by other groups [ 25 , 26 , 27 , 31 , 35 , 36 , 49 ].
Overall, the analysis of the kits performed here acts as a probe that the determination methodology needs to be carefully assayed and critically analysed as this is the ultimate guarantee of the validity of the data. Because we have already done so with the 4 kit references listed in this study, we would like to encourage researchers to share their internal validation data with other kits they might have been using, as well as to invite the companies to share more details about their products, as we believe it has been a huge limitation in the field and this would produce a significant advance, saving a lot of time and money to the research.
Throughout the literature many different studies have acknowledged the reported short half-life of CGRP [ 38 , 52 , 55 , 56 , 82 ] as a main limitation for their works. Still, many fail to describe precisely enough their methodology for sample processing so readers can infer how this limitation took place. This problem has been pointed out before and the latest works have included a more accurate description of the sample processing [ 35 , 36 , 38 , 55 ]. To avoid this rapid degradation of the peptide Messlinger et al. [ 55 ] proposed buffering the sample with peptidase inhibitor, but they concluded that immediate freezing was the most effective way to preserve CGRP content.
We did not add peptidase inhibitors as we were using serum as sample and the addition of a peptidase inhibitor needed to be done right after centrifugation but we opt to freeze the samples immediately. Our results show that the degradation of the peptide did not happen, at least in the first 24 h, when samples were stored at 4°C. This complies with the instructions of most of the ELISA kits our group has assayed and which provide a window of time for sample storage depending on the temperature, specifying that samples can be stored at 4°C for up to 24 h before being analysed. These data appear to be contradicting the results of Kraenzlin et al. [ 78 ] regarding the half-life of CGRP. One could argue that the content of serum and plasma is different and the differences found in these studies could be accounted for the binding of CGRP to cellular compartments or to fibrinogen, effectively modifying its degradation. However, the cited article, performed in 1985, is not exempt from limitations and should be reconsidered when analysing the stability of the peptide, at least in isolated biological fluids. First, this pharmacokinetic (PK) study fails to achieve some critical points that are currently required for this kind of works [ 83 ]. CGRP concentration should achieve a steady state in order to be able to extrapolate the half-life as it at this point when the phenomena of absorption, distribution, metabolism and excretion have reached and equilibrium and therefore stopping the infusion will give the information about the actual elimination half-life. Moreover, results from human in-vivo PK studies are not necessarily equivalent to those obtained from in-vitro or animal models in-vivo [ 84 ]. Our findings show that serum freezing does not need to be immediate as long as it is kept in the fridge after instant centrifugation following the clotting. This discovery has the potential to ease the methodology of sample processing for CGRP determinations. Although this is a disruptive finding, data should come with no surprise as other neuropeptides with similar and even shorter half-life than CGRP, such as vasoactive intestinal peptide (VIP) [ 85 ], amylin [ 86 ], and pituitary adenylate cyclase activating peptide-38 (PACAP-38) [ 87 ] are being measured without controversy over the sample processing time [ 33 , 51 , 88 ].
Another point recurrently mentioned in the literature is the long-term stability of the molecules when frozen. Available data indicates that storages of 8 months [ 55 ] significantly decrease the concentration of CGRP. Our results show that storages over 6 months have a decreasing effect on the serum levels of both isoforms of the peptide. With all the evidences collected future research should specify the time samples remained stored prior to being assayed as this could be a main limitation of the study and to date this data is not usually displayed. This opens up the question about whether controls should be matched not only by age and sex but also by the time their samples remained stored until measured, meaning that both groups, patients and controls, should be enrolled simultaneously to ensure the comparability of their CGRP measurements. This point has already been discussed in studies employing CGRP measurements with controversy results where cases and controls were recruited in two different time frames [ 89 ].
The first potential association between physical exercise and CGRP was described by Wyon et al. [ 90 ] with an animal model showing that rats had higher concentrations of CGRP in urine, CSF and serum after 1-h of running. Subsequent studies with more animal models have confirmed this relationship [ 91 , 92 ]. To date the evidence derived from studies with humans is scarce, with only two works [ 76 , 77 ]. The first one [ 76 ] showed that CGRP increased its concentration in samples collected by microdialysis in 8 individuals who had been subjected to eccentric exercise. In the second, completion of a half marathon produced an immediate CGRP increase dependent on the running intensity in 48 individuals [ 77 ].
The relevance for these discoveries in clinical practise is limited because subjects do not usually perform that kind of exercises right before a blood sampling. This is why we analysed the effect of exercise in a way that would reflect more accurately what might be happening at the actual sampling. The results showed that this kind of practise does not have an effect on alpha nor beta-CGRP levels and consequently the patients do not need to be on a strict rest prior to the blood extraction. However, data need to be managed carefully because the exact amount of exercise that has an effect has not been described yet and because the window between the no effect of a 20 min run and a half marathon is wide.
All the results obtained from the experimental analysis would need to be further explored with a bigger number of participants and to be tested in other samples sources that are being considered for CGRP determinations. Nonetheless, it is important to highlight that when considering the future use of CGRP as a biomarker it is necessary to select a sample source that is easy to obtain, which does not have irregular fluctuations associated with unknown factors and which offers reproducible and robust results. Jugular blood, tear fluid, CSF, GCF are not easy to obtain and saliva sampling has to follow very strict protocols to be reliable [ 93 ], so our opinion is that future research should perhaps be focusing in plasma and serum from peripheral blood.
In-house meta-analysis
Our results show that, with a huge number of participants, the levels obtained with Abbexa and CUSABIO kits fit the consensus range seen in the literature review for alpha and beta-CGRP, respectively, and contribute to set a more standardized range of concentration for the peptides.
The effects of sex and age on the circulating levels of CGRP is a point which has not been explored deeply enough. While some studies affirm that CGRP can correlate with age [ 38 ], others do not find such correlation [ 35 , 70 ]. For the data obtained from our in-house samples we found that beta-CGRP correlated positively with age, contradicting previous results obtained with the same kit in plasma and saliva [ 35 ]. Besides, the sub-group comprised by males had different alpha-CGRP content that the female, a finding which had not been described. Taking all these data together, the results call for a stricter control of the group design, which would need to be carefully matched in terms of sex and age, to avoid the effect that these two parameters could have on the comparisons.
Also, as the discrimination between alpha and beta-CGRP in research papers has recently begun [ 38 , 69 , 70 , 71 ], we have shown that these two peptides do not correlate their circulating levels and therefore the results obtained from measuring one or the other are not interchangeable and could lead to opposite conclusions because these molecules can have different behaviours even within the same disorder [ 38 ].
Strengths and limitations
Our work has several strengths. Our literature review summarizes in an easy to understand way all the mess regarding CGRP measurements, showing all the differences not only in terms of results, but also in their aims, design, measuring methodologies and conclusions, allowing for a critical analysis and which will serve as a basis for future comparisons.
Due recent literature has begun to differentiate between alpha and beta-CGRP, we have performed all our experiments to continue doing so, in an effort to expand the knowledge about the different traits of the two molecules.
All the enrolled individuals of the analysis of exercising and duration of the sample processing had their blood extraction performed at the same day and time, limiting the variability that the circadian cycle might have on the levels of the peptide, and all of them were carried out at our laboratory facilities, ensuring an immediate processing and freeze of the serum. Samples for the long-term storage analysis were also obtained at the same time of the day and all of them were collected within a week and assayed for the first and the second time altogether, limiting the effects of different storage time until the determinations and intra-assay variations.
Nonetheless, it has also some limitations that need to be listed. Although we had a bigger list of ELISA kits that have been employed by other researchers, we could not test them all and we decided to probe only 4, including both competitive and sandwich ELISA targeting total, alpha and beta-CGRP. The validity of other kits apart from the ones included in this study would need to be evaluated separately. Also, the results derived from our methodological experiments should be tested in other samples sources as we only included serum because this is, in our opinion, the best sample source for CGRP determinations. For the analysis of our data base, we acknowledge that we did not account for some of the comorbidities of the patients when analysing the effects of sex and age, but because these samples were from our bio-bank their clinical information was limited to the original aim why they were obtained and therefore did not allow such kind of correction.
We have reviewed the different results obtained throughout the years measuring CGRP making an effort to highlight their differences in terms of aim, inclusion/exclusion criteria, methodology, data display and conclusions. We have also analysed the way these differences might have affect the CGRP levels reported and we have come to the conclusion that is not only the sample or the method (RIA or ELISA) but even the brand employed which ultimately determine the concentration range.
Finally, we have illustrated some new features of CGRP determinations in serum which are very valuable for the planning of future studies. Concentrations of alpha-CGRP and beta-CGRP seems to be about (median with IQR) 37–5 (28.2–54.4) pg/mL and 4.6 (2.4–6.4) pg/mL, respectively, according to our in-house analysis, which agrees with what can be seen from the literature review. The facts that serum kept refrigerated conserves the CGRP content up to 24 h and that moderate exercise does not exert a modulation effect on the concentrations will ease the design of sample extraction and processing protocols. Also, we point out that storage time should be controlled as a new way to ensure the validity of results, probably by the simultaneous enrolling of all the subjects included in the study and/or by assaying their samples within similar time-ranges from the extraction. Ultimately, we have shown that alpha and beta-CGRP should be analysed separately as the isoforms do not correlate their concentrations and it has been illustrated in the literature that these can have different behaviours within the same disorder.
Overall, this work has brought new methodological data to progress in our way to evaluate the actual role of CGRP as a migraine biomarker at the same time it has evaluated the previous advances with a critical point of view, trying to produce a constructive criticism that will help to progress in this challenging topic.
Availability of data and materials
No datasets were generated or analysed during the current study.
Abbreviations
Bicinchoninic acid protein assay
Chronic daily headache
Calcitonin gene-related peptide
Confidence interval
Chronic migraine
Combined contraception
Cerebrospinal fluid
Cubital vein
Enzyme immune assay
Enzyme-linked immunosorbent assay
Episodic migraine
Gingival crevicular fluid
Healthy controls
International classification of headache disorders 3rd edition
Interquartile range
Jugular vein
Migraine with aura
Medication overuse
Migraine without aura
Pituitary adenylate cyclase activating peptide-38
Pharmacokinetics
Post menopause
Radioimmuno assay
Regular menstrual cycle
Standard deviation
Standard error of mean
Vasoactive intestinal peptide
Without aura
Olesen J (2018) Headache Classification Committee of the International Headache Society (IHS) The International Classification of Headache Disorders, 3rd edition. Cephalalgia 38:1–211
Hong J Bin, Lange KS, Overeem LH, et al (2023) A Scoping Review and Meta-Analysis of Anti-CGRP Monoclonal Antibodies: Predicting Response. Pharmaceuticals 16:934. https://doi.org/10.3390/ph16070934
Zobdeh F, ben Kraiem A, Attwood MM, et al (2021) Pharmacological treatment of migraine: Drug classes, mechanisms of action, clinical trials and new treatments. Br J Pharmacol 178:4588–4607
Article CAS PubMed Google Scholar
Hepp Z, Dodick DW, Varon SF et al (2015) Adherence to oral migraine-preventive medications among patients with chronic migraine. Cephalalgia 35:478–488. https://doi.org/10.1177/0333102414547138
Article PubMed Google Scholar
Edvinsson L, Haanes KA, Warfvinge K, DiN K (2018) CGRP as the target of new migraine therapies - Successful translation from bench to clinic. Nat Rev Neurol 14:338–350. https://doi.org/10.1038/s41582-018-0003-1
Gago-Veiga J-M, MGEAPGPMMÁG-G, Castañeda S, (2022) Treatment of migraine with monoclonal antibodies. Expert Opin Biol Ther 22:707–716. https://doi.org/10.1080/14712598.2022.2072207
Negro A, Martelletti P (2019) Gepants for the treatment of migraine. Expert Opin Investig Drugs 28:555–567. https://doi.org/10.1080/13543784.2019.1618830
Angus-Leppan H (2013) Migraine: mimics, borderlands and chameleons. Pract Neurol 13:308–318. https://doi.org/10.1136/practneurol-2012-000502
Amara SG, Jonas V, Rosenfeld MG, et al (1982) Alternative RNA processing in calcitonin gene expression generates mRN As encoding different polypeptide products. Nature 298:240–244. https://doi.org/10.1038/298240a0
Brain SD, Macintyre lAIN, Williams TJ, et al (1986) A second form of human calcitonin gene-related peptide which is a potent vasodilator. Eur J Phamacol 124:349–352. https://doi.org/10.1016/0014-2999(86)90238-4
Russo AF, Hay DL (2023) CGRP physiology, pharmacology, and therapeutic targets: migraine and beyond. Physiol Rev 103:1565–1644
Schütz B, Mauer D, Salmon AM et al (2004) Analysis of the cellular expression pattern of β-CGRP in α-CGRP-deficient mice. J Comp Neurol 476:32–43. https://doi.org/10.1002/cne.20211
Mulderry PK, Ghatei MA, Spokes RA et al (1988) Differential expression of α-CGRP and β-CGRP by primary sensory neurons and enteric autonomic neurons of the rat. Neuroscience 25:195–205. https://doi.org/10.1016/0306-4522(88)90018-8
Goadsby PJ, Edvinsson L, Ekman R (1990) Vasoactive peptide release in the extracerebral circulation of humans during migraine headache. Ann Neurol 28:183–187. https://doi.org/10.1002/ana.410280213
Gallai V, Sarchielli P, Floridi A, et al (1995) Vasoactive peptide levels in the plasma of young migraine patients with and without aura assessed both interictally and ictally. Cephalalgia 15:384–390. https://doi.org/10.1046/j.1468-2982.1995.150538
Sarchielli P, Alberti A, Codini M et al (2000) Nitric oxide metabolites, prostaglandins and trigeminal vasoactive peptides in internal jugular vein blood during spontaneous migraine attacks. Cephalalgia 20:907–918
Ashina M, Bendtsen L, Jensen R, et al (2000) Evidence for increased plasma levels of calcitonin gene-related peptide in migraine outside of attacks. Pain 83:133–138. https://doi.org/10.1016/s0304-3959(00)00232-3
Sarchielli P, Alberti A, Floridi A, Gallai V (2001) Levels of nerve growth factor in cerebrospinal fluid of chronic daily headache patients. Neurology 57:132–134. https://doi.org/10.1212/WNL.57.1.132
Gallai V, Alberti A, Gallai B, et al (2003) Glutamate and nitric oxide pathway in chronic daily headache: evidence from cerebrospinal fluid. Cephalalgia 23:166–174. https://doi.org/10.1046/j.1468-2982.2003.00552.x
Bellamy JL, Cady RK, Durham PL (2006) Salivary levels of CGRP and VIP in rhinosinusitis and migraine patients. Headache 46:24–33. https://doi.org/10.1111/j.1526-4610.2006.00294.x
Fusayasu E, Kowa H, Takeshima T et al (2007) Increased plasma substance P and CGRP levels, and high ACE activity in migraineurs during headache-free periods. Pain 128:209–214. https://doi.org/10.1016/j.pain.2006.09.017
Sarchielli P, Pini LA, Coppola F et al (2007) Endocannabinoids in chronic migraine: CSF findings suggest a system failure. Neuropsychopharmacology 32:1384–1390. https://doi.org/10.1038/sj.npp.1301246
Jang M-U, Park J-W, Kho H-S et al (2011) Plasma and saliva levels of nerve growth factor and neuropeptides in chronic migraine patients. Oral Dis 17:187–193. https://doi.org/10.1111/j.1601-0825.2010.01717.x
Rodríguez-Osorio X, Sobrino T, Brea D et al (2012) Endothelial progenitor cells: A new key for endothelial dysfunction in migraine. Neurology 79:474–479. https://doi.org/10.1212/WNL.0b013e31826170ce
Cernuda-Morollón E, Larrosa D, Ramón C et al (2013) Interictal increase of CGRP levels in peripheral blood as a biomarker for chronic migraine. Neurology 81:1191–1196. https://doi.org/10.1212/WNL.0b013e3182a6cb72
Cernuda-Morollõn E, Martínez-Camblor P, Ramõn C et al (2014) CGRP and VIP levels as predictors of efficacy of onabotulinumtoxin type A in chronic migraine. Headache 54:987–995. https://doi.org/10.1111/head.12372
Fekrazad R, Sardarian A, Azma K et al (2018) Interictal levels of calcitonin gene related peptide in gingival crevicular fluid of chronic migraine patients. Neurol Sci 39:1217–1223. https://doi.org/10.1007/s10072-018-3340-3
Domínguez C, Vieites-Prado A, Pérez-Mato M et al (2018) CGRP and PTX3 as Predictors of Efficacy of Onabotulinumtoxin Type A in Chronic Migraine: An Observational Study. Headache 58:78–87. https://doi.org/10.1111/head.13211
Leira Y, Ameijeira P, Domínguez C et al (2019) Periodontal inflammation is related to increased serum calcitonin gene-related peptide levels in patients with chronic migraine. J Periodontol 90:1088–1095. https://doi.org/10.1002/JPER.19-0051
Han D (2019) Association of serum levels of calcitonin gene-related peptide and cytokines during migraine attacks. Ann Indian Acad Neurol 22:277–281. https://doi.org/10.4103/aian.AIAN_371_18
Article PubMed PubMed Central Google Scholar
Kamm K, Straube A, Ruscheweyh R (2019) Calcitonin gene-related peptide levels in tear fluid are elevated in migraine patients compared to healthy controls. Cephalalgia 39:1535–1543. https://doi.org/10.1177/0333102419856640
Pérez-Pereda S, Toriello-Suárez M, Ocejo-Vinyals G et al (2020) Serum CGRP, VIP, and PACAP usefulness in migraine: a case–control study in chronic migraine patients in real clinical practice. Mol Biol Rep 47:7125–7138. https://doi.org/10.1007/s11033-020-05781-0
Irimia P, Martínez-Valbuena I, Mínguez-Olaondo A et al (2021) Interictal amylin levels in chronic migraine patients: A case-control study. Cephalalgia 41:604–612. https://doi.org/10.1177/0333102420977106
Vural S, Albayrak L (2022) Can calcitonin gene-related peptide (CGRP) and pentraxin-3 (PTX-3) be useful in diagnosing acute migraine attack? J Recept Signal Transduction 42:562–566. https://doi.org/10.1080/10799893.2022.2097264
Article CAS Google Scholar
Alpuente A, Gallardo VJ, Asskour L et al (2022) Salivary CGRP can monitor the different migraine phases: CGRP (in)dependent attacks. Cephalalgia 42:186–196
Alpuente A, Gallardo VJ, Asskour L et al (2022) Salivary CGRP and erenumab treatment response: towards precision medicine in migraine. Ann Neurol 92:846–859. https://doi.org/10.1002/ana.26472
Liu J, Wang G, Dan Y, Liu X (2022) CGRP and PACAP-38 play an important role in diagnosing pediatric migraine. J Headache Pain 23:1–13. https://doi.org/10.1186/s10194-022-01435-7
Gárate G, González-Quintanilla V, González A et al (2023) Serum Alpha and Beta-CGRP Levels in chronic migraine patients before and after monoclonal antibodies against CGRP or its receptor. Ann Neurol 94:285–294. https://doi.org/10.1002/ana.26658
Goadsby PJ, Edvinsson L (1993) The Trigreminovascular System and Migraine: Studies Characterizing Cerebrovascular and Neuropeptide Changes Seen in Humans and Cats. Annals of Neurology 33:48–56. https://doi.org/10.1002/ana.410330109
Juhasz G, Zsombok T, Jakab B, et al (2005) Sumatriptan causes parallel decrease in plasma calcitonin gene-related peptide (CGRP) concentration and migraine headache during nitroglycerin induced migraine attack. Cephalalgia 25:179–183. https://doi.org/10.1111/j.1468-2982.2005.00836.x
Sarchielli P, Pini LA, Zanchin G et al (2006) Clinical-biochemical correlates of migraine attacks in rizatriptan responders and non-responders. Cephalalgia 26:257–265. https://doi.org/10.1111/j.1468-2982.2005.01016.x
Cady RK, Vause CV, Ho TW et al (2009) Elevated saliva calcitonin gene-related peptide levels during acute migraine predict therapeutic response to rizatriptan. Headache 49:1258–1266. https://doi.org/10.1111/j.1526-4610.2009.01523.x
Cady R, Turner I, Dexter K et al (2014) An exploratory study of salivary calcitonin gene-related peptide levels relative to acute interventions and preventative treatment with onabotulinumtoxinA in chronic migraine. Headache 54:269–277. https://doi.org/10.1111/head.12250
Cernuda-Morollón E, Ramón C, Martínez-Camblor P et al (2015) OnabotulinumtoxinA decreases interictal CGRP plasma levels in patients with chronic migraine. Pain 156:820–824. https://doi.org/10.1097/j.pain.0000000000000119
Lassen LH, Haderslev PA, Jacobsen VB et al (2002) CGRP may play a causative role in migraine. Cephalalgia 22:54–61. https://doi.org/10.1046/j.1468-2982.2002.00310.x
Nicolodi M, Bianco E Del (1990) Sensory neuropeptides (substance P, calcitonin gene-related peptide) and vasoactive intestinal polypeptide in human saliva: their pattern in migraine and cluster headache. Cephalalgia 10:39–50. https://doi.org/10.1046/j.1468-2982.1990.1001039.x
Friberg L, Olesen J, Skyhøi Olsen T et al (1994) Absence of vasoactive peptide release from brain to cerebral circulation during onset of migraine with aura. Cephalalgia 14:47–54
Tvedskov JF, Lipka K, Ashina M et al (2005) No increase of calcitonin gene-related peptide in jugular blood during migraine. Ann Neurol 58:561–568. https://doi.org/10.1002/ana.20605
Lee MJ, Lee SY, Cho S, et al (2018) Feasibility of serum CGRP measurement as a biomarker of chronic migraine: a critical reappraisal. Journal of Headache and Pain 19:. https://doi.org/10.1186/s10194-018-0883-x
Latif R, Rafique N, Al AL et al (2021) Diagnostic accuracy of serum calcitonin gene-related peptide and apolipoprotein e in migraine: A preliminary study. Int J Gen Med 14:851–856. https://doi.org/10.2147/IJGM.S303350
Hanci F, Kilinc YB, Kilinc E et al (2021) Plasma levels of vasoactive neuropeptides in pediatric patients with migraine during attack and attack-free periods. Cephalalgia 41:166–175. https://doi.org/10.1177/0333102420957588
de Vries Lentsch S, Garrelds IM, Danser AHJ, et al (2022) Serum CGRP in migraine patients using erenumab as preventive treatment. J Headache Pain 23. https://doi.org/10.1186/s10194-022-01483-z
Goldstein ED, Gopal N, Badi MK et al (2023) CGRP, Migraine, and Brain MRI in CADASIL: A Pilot Study. Neurologist 28:231–236. https://doi.org/10.1097/NRL.0000000000000478
Neyal A, Ekmekyapar Fırat Y, Çekmen MB et al (2023) Calcitonin gene-related peptide and adrenomedullin levels during ictal and interictal periods in patients with migraine. Cureus. https://doi.org/10.7759/cureus.37843
Messlinger K, Vogler B, Kuhn A et al (2021) CGRP measurements in human plasma – a methodological study. Cephalalgia 41:1359–1373. https://doi.org/10.1177/03331024211024161
Kamm K (2022) CGRP and Migraine: What Have We Learned From Measuring CGRP in Migraine Patients So Far? Front Neurol 13:. https://doi.org/10.3389/fneur.2022.930383
Greco R, De Icco R, Demartini C, et al (2020) Plasma levels of CGRP and expression of specific microRNAs in blood cells of episodic and chronic migraine subjects: towards the identification of a panel of peripheral biomarkers of migraine? J Headache Pain 21. https://doi.org/10.1186/s10194-020-01189-0
Raffaelli B, Overeem LH, Mecklenburg J et al (2021) Plasma calcitonin gene-related peptide (CGRP) in migraine and endometriosis during the menstrual cycle. Ann Clin Transl Neurol 8:1251–1259. https://doi.org/10.1002/acn3.51360
Article CAS PubMed PubMed Central Google Scholar
Raffaelli B, Storch E, Overeem LH et al (2023) Sex hormones and calcitonin gene-related peptide in women with migraine: a cross-sectional, matched cohort study. Neurology 100:E1825–E1835. https://doi.org/10.1212/WNL.0000000000207114
Frank F, Kaltseis K, Messlinger K, Broessner G (2022) Short Report of Longitudinal CGRP-Measurements in Migraineurs During a Hypoxic Challenge. Front Neurol 13. https://doi.org/10.3389/fneur.2022.925748
Raffaelli B, Terhart M, Fitzek MP et al (2023) Change of CGRP plasma concentrations in migraine after discontinuation of CGRP-(Receptor) monoclonal antibodies. Pharmaceutics 15:1–9. https://doi.org/10.3390/pharmaceutics15010293
Etefagh HH, Shahmiri SS, Melali H et al (2022) Bariatric surgery in migraine patients: CGRP level and weight loss. Obes Surg 32:3635–3640. https://doi.org/10.1007/s11695-022-06218-2
Juhasz G, Zsombok T, Modos EA et al (2003) NO-induced migraine attack: Strong increase in plasma calcitonin gene-related peptide (CGRP) concentration and negative correlation with platelet serotonin release. Pain 106:461–470. https://doi.org/10.1016/j.pain.2003.09.008
Pellesi L, Al-Karagholi MAM, De Icco R, et al (2022) Plasma Levels of CGRP During a 2-h Infusion of VIP in Healthy Volunteers and Patients With Migraine: An Exploratory Study. Front Neurol 13. https://doi.org/10.3389/fneur.2022.871176
Guo S, Vollesen ALH, Hansen YBL et al (2017) Part II: Biochemical changes after pituitary adenylate cyclase-activating polypeptide-38 infusion in migraine patients. Cephalalgia 37:136–147. https://doi.org/10.1177/0333102416639517
Abbas A, Moustafa R, Shalash A et al (2022) Serum CGRP changes following ultrasound-guided bilateral greater-occipital-nerve block. Neurol Int 14:199–206. https://doi.org/10.3390/neurolint14010016
Riesco N, Cernuda-Morollón E, Martínez-Camblor P et al (2017) Relationship between serum levels of VIP, but not of CGRP, and cranial autonomic parasympathetic symptoms: A study in chronic migraine patients. Cephalalgia 37:823–827. https://doi.org/10.1177/0333102416653232
Babapour M, Khorvash F, Rouhani MH, et al (2022) Effect of soy isoflavones supplementation on migraine characteristics , mental status and calcitonin gene - related peptide ( CGRP ) levels in women with migraine : results of randomised controlled trial. Nutr J 1–11. https://doi.org/10.1186/s12937-022-00802-z
Gárate G, Toriello M, González-Quintanilla V, et al (2023) Serum alpha-CGRP levels are increased in COVID-19 patients with headache indicating an activation of the trigeminal system. BMC Neurol 23. https://doi.org/10.1186/s12883-023-03156-z
Gárate G, Pascual M, Rivero M, et al (2023) Serum Calcitonin Gene-Related Peptide α and β Levels are Increased in COVID-19 Inpatients. Arch Med Res 54. https://doi.org/10.1016/j.arcmed.2022.12.002
Gárate G, Pascual M, Olmos JM, et al (2022) Increase in Serum Calcitonin Gene-Related Peptide β (CGRPβ) Levels in COVID-19 Patients with Diarrhea: An Underlying Mechanism? Dig Dis Sci 67. https://doi.org/10.1007/s10620-022-07473-0
Alhabbab RY (2018) Radioimmunoassay (RIA). Basic Serological Testing. Springer International Publishing, Cham, pp 77–81
Chapter Google Scholar
Sadat TM, Ahmed M (2022) Enzyme-Linked Immunosorbent Assay (ELISA). In: Christian SL (ed) Cancer Cell Biology: Methods and Protocols. Springer, US, New York, NY, pp 115–134
Google Scholar
Wimalawansa SJ (1991) Circadian variation of plasma calcitonin gene-related peptide in man. J Neuroendocrinol 3:319–322. https://doi.org/10.1111/j.1365-2826.1991.tb00281.x
de Vries LS, Rubio-Beltrán E, MaassenVanDenBrink A (2021) Changing levels of sex hormones and calcitonin gene-related peptide (CGRP) during a woman’s life: Implications for the efficacy and safety of novel antimigraine medications. Maturitas 145:73–77. https://doi.org/10.1016/j.maturitas.2020.12.012
Jonhagen S, Ackermann P, Saartok T, Renstrom PA (2006) Calcitonin gene related peptide and neuropeptide Y in skeletal muscle after eccentric exercise: A microdialysis study. Br J Sports Med 40:264–267. https://doi.org/10.1136/bjsm.2005.022731
Tarperi C, Sanchis-Gomar F, Montagnana M et al (2020) Effects of endurance exercise on serum concentration of calcitonin gene-related peptide (CGRP): A potential link between exercise intensity and headache. Clin Chem Lab Med 58:1707–1712. https://doi.org/10.1515/cclm-2019-1337
Kraenzlin ME, Ch’ng JLC, Mulderry PK, et al (1985) Infusion of a novel peptide, calcitonin gene-related peptide (CGRP) in man. Pharmacokinetics and effects on gastric acid secretion and on gastrointestinal hormones. Regul Pept 10:189–197. https://doi.org/10.1016/0167-0115(85)90013-8
Reich A, Orda A, Wiśnicka B, Szepietowski JC (2007) Plasma concentration of selected neuropeptides in patients suffering from psoriasis. Exp Dermatol 16:421–428. https://doi.org/10.1111/j.1600-0625.2007.00544.x
Smillie SJ, Brain SD (2011) Calcitonin gene-related peptide (CGRP) and its role in hypertension. Neuropeptides 45:93–104
Li FJ, Zou YY, Cui Y et al (2013) Calcitonin gene-related peptide is a promising marker in ulcerative colitis. Dig Dis Sci 58:686–693. https://doi.org/10.1007/s10620-012-2406-y
Edvinsson L, Ekman R, Goadsby PJ (2010) Measurement of vasoactive neuropeptides in biological materials: Problems and pitfalls from 30 years of experience and novel future approaches. Cephalalgia 30:761–766
Krause A, Lott D, Dingemanse J (2021) Estimation of attainment of steady-state conditions for compounds with a long half-life. J Clin Pharmacol 61:82–89. https://doi.org/10.1002/jcph.1701
Cho HY, Choi GW, Lee YB (2019) Interpretation of non-clinical data for prediction of human pharmacokinetic parameters: In vitro-in vivo extrapolation and allometric scaling. Pharmaceutics 11. https://doi.org/10.3390/pharmaceutics11040168
Domschke S, Domschke W, Bloom2 SR, et al (1978) Vasoactive intestinal peptide in man: pharmacokinetics, metabolic and circulatory effects. Gut 19:1049–1053. https://doi.org/10.1136/gut.19.11.1049
Mathiesen DS, Lund A, Holst JJ et al (2022) Amylin and calcitonin – physiology and pharmacology. Eur J Endocrinol 186:R93–R111
Birk S, Sitarz JT, Petersen KA et al (2007) The effect of intravenous PACAP38 on cerebral hemodynamics in healthy volunteers. Regul Pept 140:185–191. https://doi.org/10.1016/j.regpep.2006.12.010
Al-Keilani MS, Almomani BA, Al-Sawalha NA et al (2022) Significance of serum VIP and PACAP in multiple sclerosis: an exploratory case–control study. Neurol Sci 43:2621–2630. https://doi.org/10.1007/s10072-021-05682-5
Ochoa-Callejero L, García-Sanmartín J, Villoslada-Blanco P, et al (2021) circulating levels of calcitonin gene-related peptide are lower in COVID-19 patients. J Endocr Soc 5. https://doi.org/10.1210/jendso/bvaa199
Wyon Y, Hammar M, Theodorsson E, Lundeberg T (1998) Effects of physical activity and acupuncture on calcitonin gene-related peptide immunoreactivity in different parts of the rat brain and in cerebrospinal fluid, serum and urine. Acta Physiol Scand 162:517–522. https://doi.org/10.1046/j.1365-201X.1998.0317e.x
Parnow A, Gharakhanlou R, Gorginkaraji Z, et al (2012) Effects of endurance and resistance training on calcitonin gene-related peptide and acetylcholine receptor at slow and fast twitch skeletal muscles and sciatic nerve in male wistar rats. Int J Pept 2012. https://doi.org/10.1155/2012/962651
Kooshki R, Abbasnejad M, Shamsizadeh A, et al (2020) Physical exercise enhances vulnerability to migraine headache associated with CGRP up-expression in trigeminal nucleus caudalis of stressed rats. Neurol Res 42:952–958. https://doi.org/10.1080/01616412.2020.1794243
Jasim H, Carlsson A, Hedenberg-Magnusson B, et al (2018) Saliva as a medium to detect and measure biomarkers related to pain. Sci Rep 8. https://doi.org/10.1038/s41598-018-21131-4
Download references
Acknowledgements
Not applicable.
This study has been founded by Instituto de Salud Carlos III (ISCII) through the project PI20/01358, co-funded by Fondos Europeos de Desarrollo Regional (FEDER), “Una manera de hacer Europa”, and through the project PMP22/00183, co-founded by the Recovery and Resilience Plan by The European Union NextGenerationUE.
Author information
Authors and affiliations.
Instituto de Investigación Marqués de Valdecilla (IDIVAL), Hospital Universitario Marqués de Valdecilla & Universidad de Cantabria, Santander, Spain
Gabriel Gárate, Julio Pascual, Marta Pascual-Mato, Jorge Madera, María Muñoz-San Martín & Vicente González-Quintanilla
You can also search for this author in PubMed Google Scholar
Contributions
GG, VGQ, JP designed the study, collected and analysed the data and wrote the manuscript. VGQ, JM, MPM and JP recruited participants for the study. All authors reviewed, contributed, and edited the final draft. All authors approved the final version.
Corresponding author
Correspondence to Gabriel Gárate .
Ethics declarations
Ethics approval and consensus to participate.
The study was approved by the Ethics Committee of Cantabria and its approval has been published in the record 28/2020 of December 11, 2020. All participants gave written informed consent for their inclusion in the study.
Consent for publication
Competing interests.
The authors declare no competing interests.
Additional information
Publisher’s note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ . The Creative Commons Public Domain Dedication waiver ( http://creativecommons.org/publicdomain/zero/1.0/ ) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
Reprints and permissions
About this article
Cite this article.
Gárate, G., Pascual, J., Pascual-Mato, M. et al. Untangling the mess of CGRP levels as a migraine biomarker: an in-depth literature review and analysis of our experimental experience. J Headache Pain 25 , 69 (2024). https://doi.org/10.1186/s10194-024-01769-4
Download citation
Received : 18 March 2024
Accepted : 09 April 2024
Published : 29 April 2024
DOI : https://doi.org/10.1186/s10194-024-01769-4
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
The Journal of Headache and Pain
ISSN: 1129-2377
- Submission enquiries: [email protected]
- Open access
- Published: 30 April 2024
Extent, transparency and impact of industry funding for pelvic mesh research: a review of the literature
- Angela Coderre-Ball 1 &
- Susan P. Phillips ORCID: orcid.org/0000-0003-4798-1742 1 , 2
Research Integrity and Peer Review volume 9 , Article number: 4 ( 2024 ) Cite this article
111 Accesses
2 Altmetric
Metrics details
Conflicts of interest inherent in industry funding can bias medical research methods, outcomes, reporting and clinical applications. This study explored the extent of funding provided to American physician researchers studying surgical mesh used to treat uterine prolapse or stress urinary incontinence, and whether that funding was declared by researchers or influenced the ethical integrity of resulting publications in peer reviewed journals.
Publications identified via a Pubmed search (2014–2021) of the terms mesh and pelvic organ prolapse or stress urinary incontinence and with at least one US physician author were reviewed. Using the CMS Open Payments database industry funding received by those MDs in the year before, of and after publication was recorded, as were each study’s declarations of funding and 14 quality measures.
Fifty-three of the 56 studies reviewed had at least one American MD author who received industry funding in the year of, or one year before or after publication. For 47 articles this funding was not declared. Of 247 physician authors, 60% received > $100 while 13% received $100,000-$1,000,000 of which approximately 60% was undeclared. While 57% of the studies reviewed explicitly concluded that mesh was safe, only 39% of outcomes supported this. Neither the quality indicator of follow-up duration nor overall statements as to mesh safety varied with declaration status.
Conclusions
Journal editors’ guidelines re declaring conflicts of interest are not being followed. Financial involvement of industry in mesh research is extensive, often undeclared, and may shape the quality of, and conclusions drawn, resulting in overstated benefit and overuse of pelvic mesh in clinical practice.
Peer Review reports
Introduction
When medical research and vested interest collide, objectivity, research integrity, and best clinical practices are sometimes the victims. Compromise to objectivity can arise via ghost management of research [ 1 ], that is by direct involvement of industry personnel, or indirectly through industry transfers of honoraria, gratuities, or speaker payments made to independent researchers [ 2 ]. Circumstances such as these, that “create a risk that judgments or actions regarding a primary interest will be unduly influenced by a secondary interest are defined as conflicts of interest (COI)” [ 3 ]. COI stemming from industry funding can, although do not always [ 4 ], bias design, recruitment, conduct, choice of outcome measures, or reporting, all of which have the potential to distort study findings and undermine medical practice [ 5 , 6 , 7 ]. The United States Centers for Medicare & Medicaid Services Open Payments [ 8 ] database documents any industry payment of at least $10 and annual payments of $100 or more made to American physician researchers since 2013. Its creation has facilitated identifying a portion of corporate support for medical research.
We wished to examine the extent, accuracy and implications of COI reporting among authors studying the effectiveness and safety of one particular medical device, pelvic mesh. The CMS Open Payments database described above enables this examination although only for authors who were or are US physicians. Surgical mesh was first used in hernia surgery in the 1950s [ 9 ] and has become the standard of care for hernia repairs, although controversy remains [ 10 ]. By the late 1990s, surgical mesh was routinely being inserted trans-vaginally to treat pelvic organ prolapse (POP) and stress urinary incontinence (SUI). This repurposing required no approval in the US because the Food and Drug Administration’s (FDA) 510k route grants automatic authorization for products deemed to be equivalent to predicate devices already in use [ 11 , 12 ]. Prior to 1976 the FDA did not require testing of any biomedical devices, meaning surgical mesh had never undergone pre-market testing [ 13 ]. Studies of success, failure and safety of both hernia and pelvic mesh are, therefore, generally retrospective reviews tracking outcomes of use in patients.
The FDA estimates that one in eight women (in the US) undergo surgery to repair uterine prolapse [ 14 ]. Post-market evidence from peer-reviewed journals has generally endorsed pelvic mesh to be a successful treatment for POP and SUI [ 15 ]. At the same time there are reports from an unknown proportion of female mesh recipients questioning that success [ 16 , 17 ]. Commentaries have noted the close links among industry, researchers, surgeons and professional organizations that examine or voice support for pelvic mesh use [ 18 ]. Two studies of mesh used for hernia repairs raise questions about the evidence supporting its success and safety in that setting. First, despite many accounts of the value of mesh for hernia repair, none has reported on women, specifically, or considered that women’s greater immune response to foreign materials might predispose to disproportionate harm from insertion of the product [ 12 , 19 ]. Second, Sekigami and colleagues [ 20 ] determined that the majority of studies of mesh used for hernia repairs did not accurately report COI.
Whether and how industry funding is entwined with published research on pelvic mesh is unknown. As noted above, what is known is that such funding compromises medical research in general [ 21 ]. Our objectives were, therefore, to: (1) examine the scope of industry funding provided to US physician-authors of pelvic mesh research; (2) determine the proportions of that funding that were declared or undeclared and; (3) explore whether the methodologic strength and conclusions of industry funded studies differed from those without industry support.
Study selection/data extraction
We undertook a cross-sectional review of publications identified in a PubMed search in October 2021. All studies related to surgical mesh used in POP and SUI repairs were initially identified. Included were clinical trials and observational studies with at least one American physician author, and that examined post-surgical outcomes for polypropylene mesh inserted for the treatment of POP or SUI. We excluded studies with no original data, no US physician authors, those whose main purpose was to compare surgical techniques (e.g., single incision mesh vs. sacrospinous ligament fixation), studies using only autologous material or non-polypropylene mesh, and studies that only examined peri-operative outcomes.
Search terms included (POP[title/abstract] OR SUI[title/abstract]) AND mesh[title/abstract]. Studies published between January 1, 2014, and September 30, 2021 were included. This time frame matched available entries in the CMS Open Payments database (see below). We chose the year of publication rather than year of acceptance as not all studies documented their acceptance date. Included were studies from any peer-reviewed journal. One author (ACB) screened studies for inclusion/exclusion criteria, and, if questions arose, discussion occurred between the two authors.
For each study, we extracted the authors’ and journal’s names, the date of acceptance where available and of publication, conflict-of-interest statements, funding declarations, the study’s inclusion and exclusion criteria, the outcome scales or measures, outcomes, and follow-up duration. We also determined the journal’s impact factor (April 2022). This information for 10 randomly selected studies was independently abstracted by both authors who then discussed and compared results to ensure accuracy and consistency. One author then extracted data for the remaining 48 studies. These data were then reviewed by both authors, together (see Outcomes, below).
Open payments
For each physician author in each study, we searched the CMS Open Payments database to collect information on the types of payments (general, research, associated funding, and ownership and investment) made from all drug and device companies, the US dollar amount of each payment, and the companies making the payments. We included all payments authors received during the year before, the year of, and the year following publication to best ensure that all author payments that could be related to a study were captured. Payments totaling less than $100 over the three years, were entered as ‘no payment’. Small payments can influence physicians’ research and clinical behavior, however such amounts were not included to avoid modest sums or gratuities received that were likely unrelated to research.
Findings assessed
The key findings examined were the extent of industry funding of research and the dollar difference between declared and actual industry payment received. First we tallied the number of authors and papers with COI, whether declared or not. We then examined the declaration status of each author with a COI. This was recorded as no discrepancy if that COI was declared. We then counted how many authors made no declaration or declared that they did not have a COI and recorded each author’s total payment from all categories over the three years. We did not examine each journal’s declaration of COI requirements and authors’ compliance with these, nor could we determine whether aspects of authors’ declarations were redacted by specific journals.
To assess the strength of each study we examined the following. We determined the duration of patient follow-up post-surgery. This measure was chosen because complications from pelvic mesh continue to arise years after insertion. If studies did not explicitly state a mean or median follow-up in their results we accepted the follow-up duration as the timeframe indicated in the methods/design. If no measure or statement was present, this was left blank. The use of objective (e.g., POP-Q) and/or subjective (e.g., UDI-6, pain) scales and/or outcomes was tracked for each study. Critical appraisal of each included study was assessed using a purpose-built data extraction and appraisal tool (see Table 1 ) based on the Joanna Briggs Institute Checklist for Cohort Studies [ 22 ]. Fourteen questions appraised methodology including, for example, “ Are the authors conclusions supported by the findings ?” and “ Did the authors make a statement that mesh was safe to use ?” To ensure reliability both authors critically appraised each study independently and then reviewed and discussed all appraisals together to resolve differences and reach consensus. Evaluation of whether authors’ conclusions were supported by the findings (Table 1 , question ‘n’) was decided based on review of all the quality dimensions and discussion between both authors. For example, if a study made a positive conclusion about the effectiveness of mesh, but only followed patients for a short time (e.g., less than 12 months) and without a comparison group, it would be given a score of “no” or “unclear” for question ‘n’. Authors were blinded to information about funding when these quality indicators were recorded. Only after appraising and recording the strength of each study was this information merged with funding data.
Statistical analysis
Univariate analyses were used to determine the presence of study characteristics that aligned with discrepancy between declared and undeclared COI. Guided by previous research on COI of authors studying hernia mesh [ 20 ] we included impact factor (continuous), follow-up time (continuous), author’s role (e.g. first author, contributing author, senior author – categorical), and recommendations of mesh safety and effectiveness (categorical – yes/no). We report the difference in payments received between those that declared and did not declare COI. The relationship between categorical variables (e.g., author role) and the presence of undeclared COI was determined using Chi-Square testing. Logistic regression was used to determine the association of continuous variables (e.g., impact factor, follow-up time) with whether or not there was a discrepancy between reported and discovered COI (from CMS Open Payments).
Five hundred and sixty-two studies were retrieved from the PubMed search. After an initial review 56 of these were found to meet inclusion criteria (see Fig. 1 : Overview of retrieved articles, screening process, and final included studies). The majority of the excluded studies had no author whose data would appear in Open Payments (i.e. no American physician author).
Scope and declaration of industry funding: authors
There were a total of 299 authors of the 56 studies included in the full review. After excluding non-physicians and non-American physician authors as they would not be listed in the Open Payments database, 247 American MD authors remained and were included. For the remainder of the report, we only include these American MD authors in analyses.

Overview of retrieved articles, screening and final included studies
Of the 247 authors and across all 56 included studies one hundred forty-nine authors (60%) received payments totaling more than $100. Eighty-one authors’ (33%) explicit declarations that they did not have COI aligned with Open Payments documentation of payments of less than $100 over the relevant three-year timeframe examined. An additional 12 authors (5%) made no declaration and did not receive payments totaling more than $100. Twenty-eight authors (11%) explicitly declared COI and did receive more than $100 in payments. One hundred and one authors (40%) explicitly declared that they had no COI but received payments, 20 (8%) did not make any declaration and received payments, and five authors (2%) declared a conflict although no payments were recorded in Open Payments.
Examining the dollar value of payments received, we found that the largest group receiving payments (36%, n = 54) was for amounts of between $100 and $1000 and was made to authors who did not declare any COI. The remaining undeclared payments were between $1,000-$10,000 (24%, n = 36), between $10,000-$100,000 (13%, n = 20) and >$100,000 (7%, n = 11).
The majority of payments for each of the four dollar amounts were undeclared (see Fig. 2 : Proportions and amounts of declared and undeclared payments received by authors).

Proportions and amounts of declared and undeclared payments received by authors
Scope and declaration of industry funding: studies
Of the 56 studies reviewed, 53 (95%) had at least one American physician author with COI (declared or not). Thirty-nine (70%) included at least two American MD authors with COI, and 28 (54% of the 52 studies with 3 or more authors) had three or more American MD authors with COI.
Considering only non-declared COI, we found that 47 (84%) of studies included at least one American MD author with an undeclared COI, while 34 (61%) had at least two such authors, and 20 studies (38% of articles with more than 2 authors) had three or more authors with COI. Only three (5%) studies had no physician authors with any conflicts of interest (declared or not).
Study characteristics aligned with undeclared COI
We next examined alignment of the dollar amount of industry funding received and any of the following: declaring a COI; the duration of follow-up in a study; or the journal’s impact factor.
The median payment for US authors was $18,678 (IQR ~ $5000-$99,000) for those with declared COI and $158 (IQR ~ 0-$1,500) among authors, who did not declare COI, but had one (Cohen’s d effect size estimate = 0.39, 95% CI: 0.77 − 0.02).
Means and medians of the length of time patients were followed after mesh implant surgery were reported in 48/56 studies. Median follow-up was 1.0 year, with a mean of 1.9 years. Follow-up duration was not associated with whether or not a study had at least one author with undeclared COI ( OR = 0.82 95% CI:0.54 1.17). The small number of studies without COI ( n = 3) precluded comparing follow-up duration between them and the 53 with COI.
The impact factors of the journals publishing studies were also examined to see if there was any relationship with number of undeclared COI. A journal’s impact factor did not predict whether or not a study had at least one author with undeclared COI ( OR = 0.98 95%CI [0.75 1.3]).
There was a trend although no statistical association between being the lead or senior author and the presence of COI ( p = 0.18). 65% of first authors had COI (declared or not), as did 56% of middle authors, and 69% of senior authors.
Quality appraisal
We assessed the quality of each study using the 14 measures listed in Table 1 . Only 26% ( n = 14) of articles included a comparison group, partially reflecting the different study designs included in the review, and of those, 40% had comparable patients (e.g., age) in the intervention and control groups. The majority of studies (80%) did identify at least one patient characteristic such as age or obesity that could affect the success of mesh as a treatment. Only 28% ( n = 13) of these studies, however, utilized these data in their analyses. The majority of publications explicitly stated that mesh was safe and beneficial ( n = 32, 57%) although only 39% ( n = 22) of all articles’ methods and outcomes supported these conclusions (Table 1 ). The small number of studies with no COI (3 of 56) precluded comparisons of quality between groups defined by the presence or absence of COI.
95% of the 56 articles reviewed had at least one author among those who could be assessed using Open Payments who received industry funding. The majority of this funding (47/53 of articles) was undeclared. COI among American MD authors studying pelvic mesh are substantial (60%), and most (81%) are undeclared. This level of unacknowledged industry support aligns with findings of a meta-analysis of studies of undisclosed industry support to physicians in general [ 7 ] and of clinical practice guideline authors’ COI [ 23 ]. It may also explain why, despite patient reports and legal findings of harm, the scholarly literature tends to endorse pelvic mesh as effective and safe.
In 2009, the International Committee of Medical Journal Editors (ICMJE) introduced requirements for detailed disclosure of all relevant COI by any author [ 24 ]. All articles in this review were published well after this. Observed non-compliance could arise from journal laxity, researchers’ sense of impunity, conviction that they are not swayed by industry largess, or convincing themselves that funding received was not related to the reported research. 36% of all authors received undeclared industry support of less than $1000. Some might consider that smaller levels of funding which may not have been offered explicitly for research are unlikely to sway physicians and should, therefore, be exempt from required reporting. In reality, even small gifts and gratuities have repeatedly been found to ‘win over’ physicians’ research and practice [ 7 ]. In our study, industry-funding had an equivocal impact on research quality and reported outcomes. The majority of publications explicitly stated that mesh was safe and beneficial (57%, n = 32) although only 10 of those 32 substantiated this with evidence. The median follow-up time of one-year post-op would have missed long-term complications. Such complications and failures of pelvic mesh are known to arise years after its insertion. For this reason, follow-up duration was chosen as a key indicator of study validity. As most studies were retrospective chart reviews longer follow-up duration could have been built into research designs. Indicators of poor research quality did not vary with authors’ declarations of industry support. The near ubiquitous presence of industry funding, however, precluded assessment of quality differences in articles with and without COI, and left us unable to really address aim 3 of this study.
Limitations
The ability to track COI of all authors rather than only US physicians would help clarify the full extent and impact of industry funding on study design, findings, and interpretation of results. Open Payments data only include physicians licenced in the US. The database is verified and frequently updated but does not presume to include all payments made [ 25 ]. Accurate tracking of funding is further compromised because device manufacturers are known to violate reporting requirements [ 26 ]. Payments made to researchers’ family members, research or office staff, PhDs, institutions rather than individuals, etc., and any payments originating outside the US cannot, at present, be tracked. By extracting payment information for the year preceding, the year of and the year after publication we have attempted to identify all payments relevant to the articles studied, but may have missed some industry funding for included studies or captured funding for unrelated projects. It is also possible that funding received was not linked to the reviewed publication. Journal non-compliance with ICMJE requirements for declaring COI may have removed the reporting requirement for some authors and some funding. The overall impact of all these limitations may be an underestimation of the extent of undeclared industry funding to researchers.
Although we attempted to standardize our appraisal of articles, quality appraisal, as the name suggests, involves qualitative elements. The authors first rated each article separately then engaged in discussion to reach consensus, but acknowledge that the ‘objectivity’ of this process could be questioned.
Industry funding for medical research is, at present, substantial and can be a source of innovation, but needs to also be ethical and transparent. During the timeframe studied the extent of industry involvement in research explicitly justifying the merit of pelvic mesh was high, while findings were at odds with concurrent FDA warnings of risk [ 14 ]. Equally important, self-reporting of financial COI by researchers appears to be unreliable and often contravenes requirements agreed upon by international medical journal editors. Industry funding both declared and, to a greater extent, undeclared, permeates almost all research on pelvic mesh and almost certainly shapes the quality of and conclusions drawn from those studies. This biased evidence in turn skews the risk benefit picture and potentially drives overuse of pelvic mesh in clinical practice.
Availability of data and materials
All data used and generated can be made available by the corresponding author upon reasonable request.
Abbreviations
United States Centers for Medicare & Medicaid Services Open Payments
- Conflicts of interest
US Food and Drug Administration
International Committee of Medical Journal Editors
Interquartile range
Medical doctor
Pelvic organ prolapse
Stress urinary incontinence
Sismondo S, Doucet M. Publication Ethics and the Ghost Management of Medical Publication Bioethics. 2010;24(6):273–283. https://doi.org/10.1111/j.1467-8519.2008.01702.x .
Ioannidis JPA, Why Most Clinical Research Is Not Useful. PLoS Med. 2016;13(6):e1002049–1002049. https://doi.org/10.1371/journal.pmed.1002049 .
Article Google Scholar
Institute of Medicine Committee on Standards for Developing Trustworthy Clinical Practice G. Clinical practice guidelines we can trust. Washington (DC): National Academy of Sciences; 2011.
Google Scholar
Via GG, Brueggeman DA, Lyons JG, Frommeyer TC, Froehle AW, Krishnamurthy AB. Funding has no effect on studies evaluating viscosupplementation for knee osteoarthritis: a systematic review of bibliometrics and conflicts of interest. J Orthop. 2023;39:18–29. https://doi.org/10.1016/j.jor.2023.03.015 .
Ahn R, Woodbridge A, Abraham A, et al. Financial ties of principal investigators and randomized controlled trial outcomes: cross sectional study. BMJ (Online). 2017;356:i6770–6770. https://doi.org/10.1136/bmj.i6770 .
Lundh A, Lexchin J, Mintzes B, Schroll JB, Bero L. Industry sponsorship and research outcome. Cochrane Database Syst Reviews. 2017;2017(2):MR000033–000033. https://doi.org/10.1002/14651858.MR000033.pub3 .
Taheri C, Kirubarajan A, Li X, Lam ACL, Taheri S, Olivieri NF. Discrepancies in self-reported financial conflicts of interest disclosures by physicians: a systematic review. BMJ Open. 2021;11(4):e045306. https://doi.org/10.1136/bmjopen-2020-045306 .
United States Centers for Medicare & Medicaid Services. Open Payments. ( https://www.cms.gov/openpayments ).
Sanders DL, Kingsnorth AN. From ancient to contemporary times: a concise history of incisional hernia repair. Hernia: J Hernias Abdom wall Surg. 2012;16(1):1–7. https://doi.org/10.1007/s10029-011-0870-5 .
Robinson TN, Clarke JH, Schoen J, Walsh MD. Major mesh-related complications following hernia repair: events reported to the Food and Drug Administration. Surg Endosc. 2005;19(12):1556–60. https://doi.org/10.1007/s00464-005-0120-y .
Heneghan C, Aronson JK, Goldacre B, Mahtani KR, Plüddemann A, Onakpoya I. Transvaginal mesh failure: lessons for regulation of implantable devices. BMJ (Online). 2017a;359:j5515–5515. https://doi.org/10.1136/bmj.j5515 .
Phillips SP, Gee K, Wells L, Medical, Devices. Invisible women, harmful consequences. Int J Environ Res Public Health. 2022;19(21):14524. https://www.mdpi.com/1660-4601/19/21/14524 .
Heneghan CJ, Goldacre B, Onakpoya I, et al. Trials of transvaginal mesh devices for pelvic organ prolapse: a systematic database review of the US FDA approval process. BMJ open. 2017;7(12):e017125–017125. https://doi.org/10.1136/bmjopen-2017-017125 .
Food US, Administration D. FDA takes action to protect women’s health, orders manufacturers of surgical mesh intended for transvaginal repair of pelvic organ prolapse to stop selling all devices. 2019.
Rubin R. Mesh implants for women: scandal or Standard of Care? JAMA: J Am Med Association. 2019;321(14):1338–40. https://doi.org/10.1001/jama.2019.0940 .
Motamedi M, Carter SM, Degeling C. Women’s experiences of and perspectives on transvaginal mesh surgery for stress urine incontinency and pelvic organ prolapse: a qualitative systematic review. The patient: patient-. Centered Outcomes Res. 2022;15(2):157–69. https://doi.org/10.1007/s40271-021-00547-7 .
Taylor D. The failure of polypropylene surgical mesh in vivo. J Mech Behav Biomed Mater. 2018;88:370–6. https://doi.org/10.1016/j.jmbbm.2018.08.041 .
Gornall J. Vaginal mesh implants: putting the relations between UK doctors and industry in plain sight. BMJ;363:k4164. https://doi.org/10.1136/bmj.k4164 .
Klein SL, Flanagan KL. Sex differences in immune responses. Nat Rev Immunol. 2016;16(10):626–38. https://doi.org/10.1038/nri.2016.90 .
Sekigami Y, Tian T, Char S, et al. Conflicts of interest in studies related to Mesh Use in ventral hernia repair and Abdominal Wall Reconstruction. Ann Surg. 2021;276(5):e571–6. https://doi.org/10.1097/SLA.0000000000004565 .
Chimonas S, Mamoor M, Zimbalist SA, Barrow B, Bach PB, Korenstein D. Mapping conflict of interests: scoping review. BMJ. 2021;375:e066576. https://doi.org/10.1136/bmj-2021-066576 .
Moola SMZ, Tufanaru C, Aromataris E et al. Chapter 7: Systematic reviews of etiology and risk. In: Aromataris E MZ, ed. JBI Manual for Evidence Synthesis 2020.
Mooghali M, Glick L, Ramachandran R, Ross JS. Financial conflicts of interest among US physician authors of 2020 clinical practice guidelines: a cross-sectional study. BMJ open. 2023;13(1):e069115–069115. https://doi.org/10.1136/bmjopen-2022-069115 .
Drazen JM, Van Der Weyden MB, Sahni P, et al. Uniform Format for Disclosure of competing interests in ICMJE journals. JAMA: J Am Med Association. 2010;303(1):75–6. https://doi.org/10.1001/jama.2009.1542 .
Department of Health and Human Services Office of Inspector General. Open Payments Data: Review of Accuracy, Precision, and Consistency in Reporting. 2018. ( https://oig.hhs.gov/oei/reports/oei-03-15-00220.pdf ).
Adashi EY, Cohen IG. Enforcement of the Physician payments Sunshine Act: Trust and verify. JAMA: J Am Med Association. 2021;326(9):807–8. https://doi.org/10.1001/jama.2021.13156 .
Download references
Acknowledgements
Not applicable.
Funding was received from an internal Queen’s University grant (Wicked Ideas).
Author information
Authors and affiliations.
Centre for Studies in Primary Care, Queen’s University, Kingston, Canada
Angela Coderre-Ball & Susan P. Phillips
Family Medicine and Public Health Sciences, Queen’s University, Kingston, Canada
Susan P. Phillips
You can also search for this author in PubMed Google Scholar
Contributions
Both authors contributed to all aspects of the study.
Corresponding author
Correspondence to Susan P. Phillips .
Ethics declarations
Ethics approval and consent to participate.
Neither ethics approval nor consent for publication were applicable given the study design.
Consent for publication
The authors consent to publication of this paper.
Competing interests
Authors have no financial or non-financial conflicts of interest to declare.
Additional information
Publisher’s note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ . The Creative Commons Public Domain Dedication waiver ( http://creativecommons.org/publicdomain/zero/1.0/ ) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
Reprints and permissions
About this article
Cite this article.
Coderre-Ball, A., Phillips, S.P. Extent, transparency and impact of industry funding for pelvic mesh research: a review of the literature. Res Integr Peer Rev 9 , 4 (2024). https://doi.org/10.1186/s41073-024-00145-9
Download citation
Received : 18 September 2023
Accepted : 09 April 2024
Published : 30 April 2024
DOI : https://doi.org/10.1186/s41073-024-00145-9
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Pelvic mesh
- Industry funding
- Research methods
- Uterine prolapse, stress urinary incontinence, women's health
Research Integrity and Peer Review
ISSN: 2058-8615
- Submission enquiries: [email protected]
- General enquiries: [email protected]
Log in using your username and password
- Search More Search for this keyword Advanced search
- Latest content
- Current issue
- For authors
- New editors
- BMJ Journals More You are viewing from: Google Indexer
You are here
- Online First
- Best practices for the dissemination and implementation of neuromuscular training injury prevention warm-ups in youth team sport: a systematic review
- Article Text
- Article info
- Citation Tools
- Rapid Responses
- Article metrics
- http://orcid.org/0009-0005-0529-0398 Destiny Lutz 1 ,
- http://orcid.org/0000-0001-6429-4333 Carla van den Berg 1 ,
- http://orcid.org/0000-0003-3056-8169 Anu M Räisänen 1 , 2 ,
- Isla J Shill 1 , 3 ,
- Jemma Kim 4 , 5 ,
- Kenzie Vaandering 1 ,
- Alix Hayden 6 ,
- http://orcid.org/0000-0002-0427-2877 Kati Pasanen 1 , 7 , 8 , 9 ,
- http://orcid.org/0000-0002-5951-5899 Kathryn J Schneider 1 , 3 , 8 , 9 , 10 ,
- http://orcid.org/0000-0002-9499-6691 Carolyn A Emery 1 , 3 , 8 , 9 , 11 , 12 , 13 ,
- http://orcid.org/0000-0002-5984-9821 Oluwatoyosi B A Owoeye 1 , 4
- 1 Sport Injury Prevention Research Centre, Faculty of Kinesiology , University of Calgary , Calgary , Alberta , Canada
- 2 Department of Physical Therapy Education - Oregon , Western University of Health Sciences College of Health Sciences - Northwest , Lebanon , Oregon , USA
- 3 Hotchkiss Brain Institute , University of Calgary , Calgary , Alberta , Canada
- 4 Department of Physical Therapy & Athletic Training , Doisy College of Health Sciences, Saint Louis University , Saint Louis , Missouri , USA
- 5 Interdisciplinary Program in Biomechanics and Movement Science , University of Delaware College of Health Sciences , Newark , Delaware , USA
- 6 Libraries and Cultural Resources , University of Calgary , Calgary , Alberta , Canada
- 7 Tampere Research Center for Sports Medicine , Ukk Instituutti , Tampere , Finland
- 8 McCaig Institute for Bone and Joint Health , University of Calgary , Calgary , Alberta , Canada
- 9 Alberta Chilrden's Hopsital Research Institute , University of Calgary , Calgary , Alberta , Canada
- 10 Sport Medicine Centre , University of Calgary , Calgary , Alberta , Canada
- 11 O'Brien Institute for Public Health , University of Calgary , Calgary , Alberta , Canada
- 12 Department of Community Health Sciences , Cumming School of Medicine, University of Calgary , Calgary , Alberta , Canada
- 13 Department of Paediatrics , Cumming School of Medicine, University of Calgary , Calgary , Alberta , Canada
- Correspondence to Ms Destiny Lutz, Sport Injury Prevention Research Centre, Faculty of Kinesiology, University of Calgary, Calgary, Alberta, Canada; destiny.lutz{at}ucalgary.ca
Objective To evaluate best practices for neuromuscular training (NMT) injury prevention warm-up programme dissemination and implementation (D&I) in youth team sports, including characteristics, contextual predictors and D&I strategy effectiveness.
Design Systematic review.
Data sources Seven databases were searched.
Eligibility The literature search followed Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. Inclusion criteria: participation in a team sport, ≥70% youth participants (<19 years), D&I outcomes with/without NMT-related D&I strategies. The risk of bias was assessed using the Downs & Black checklist.
Results Of 8334 identified papers, 68 were included. Sport participants included boys, girls and coaches. Top sports were soccer, basketball and rugby. Study designs included randomised controlled trials (RCTs) (29.4%), cross-sectional (23.5%) and quasi-experimental studies (13.2%). The median Downs & Black score was 14/33. Injury prevention effectiveness (vs efficacy) was rarely (8.3%) prioritised across the RCTs evaluating NMT programmes. Two RCTs (2.9%) used Type 2/3 hybrid approaches to investigate D&I strategies. 19 studies (31.6%) used D&I frameworks/models. Top barriers were time restrictions, lack of buy-in/support and limited benefit awareness. Top facilitators were comprehensive workshops and resource accessibility. Common D&I strategies included Workshops with supplementary Resources (WR; n=24) and Workshops with Resources plus in-season Personnel support (WRP; n=14). WR (70%) and WRP (64%) were similar in potential D&I effect. WR and WRP had similar injury reduction (36–72%) with higher adherence showing greater effectiveness.
Conclusions Workshops including supplementary resources supported the success of NMT programme implementation, however, few studies examined effectiveness. High-quality D&I studies are needed to optimise the translation of NMT programmes into routine practice in youth sport.
Data availability statement
Data are available in a public, open access repository. Not Applicable.
https://doi.org/10.1136/bjsports-2023-106906
Statistics from Altmetric.com
Request permissions.
If you wish to reuse any or all of this article please use the link below which will take you to the Copyright Clearance Center’s RightsLink service. You will be able to get a quick price and instant permission to reuse the content in many different ways.
WHAT IS ALREADY KNOWN ON THE TOPIC
Neuromuscular training (NMT) injury prevention warm-up programmes are effective at preventing injury rates in youth sports. However, for proper dissemination and implementation (D&I) by multiple stakeholders, barriers such as low adoption, adherence and lack of time must be addressed.
WHAT THIS STUDY ADDS
There are limited high-quality research studies to facilitate the widespread adoption of, and improved adherence to, NMT programmes. Few studies used D&I theories, frameworks or models. Programme flexibility is a common barrier to implementation; adaptation of NMT programmes to fit local contexts is imperative. Comprehensive workshops and supplementary resources currently support the success of NMT programme implementation.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Promotion of NMT programmes as the standard of practice is essential to increase practical D&I of these programmes, and thus reduce the burden of youth sport injuries. This work provides some directions for stakeholders, including researchers, implementation support practitioners and youth sport policymakers, on current best practices for the delivery of NMT programmes in local youth sport settings. This work also provides the evidence base for more translational research efforts in youth sport injury prevention, a much-needed next step to optimise NMT programmes into youth sport practice.
Introduction
Youth (<19 years) sport participation provides numerous benefits, positively impacting physical and mental health. 1 Youth sport participation rates are high, with up to 90% of youth participating in sport globally. 2–5 However, with increased sport participation comes increased injury risk. One-in-three youth sustain a sport-related injury each year, leading to a significant public health burden with high healthcare costs. 3 6–8 Sport-related injuries may also result in long-term health consequences (eg, poor mental health, reduced physical activity, post-traumatic osteoarthritis). 7–9 Implementing injury prevention strategies is critical to mitigate the injury risk associated with youth sport participation.
Neuromuscular training (NMT) injury prevention warm-up programmes in youth team sport are effective in reducing injury rates by up to 60% and decreasing costs associated with injury based on randomised controlled trials (RCT) and systematic reviews. 10–21 NMT programmes include exercises that can be categorised across aerobic, balance, strength and agility components 22 23 and typically take 10–15 min. 24 25 Originally implemented with the intention of reducing non-contact lower extremity injury risk, 26–28 the effectiveness of NMT programmes has since been evaluated across numerous sports, age groups and levels of play and are associated with lower extremity and overall injury rates compared with standard of practice warm-ups. 12 20 21 25 In youth team sports, a protective effect has been demonstrated in soccer, handball, basketball, netball, rugby and floorball. 11 16 29–31 The International Olympic Committee Consensus Statement on Youth Athletic Development recommends multifaceted NMT warm-up programmes in youth sport. 32
Despite being a primary injury prevention strategy across youth sports, NMT programme adoption remains low. 33–38 For evidence-informed interventions to be successful and have a practical impact, pragmatic approaches derived from dissemination and implementation (D&I) science are necessary across multiple socioecological levels including organisation, coach and player. 36 Dissemination is defined as ‘the active process of spreading evidence-based interventions to a target population through determined channels and using planned strategies’. Implementation is ‘the active process of using strategies across multiple levels of change to translate evidence-based interventions into practice and prompt corresponding behaviour change in a target population’. 36
The aim of this systematic review was to evaluate current best practices for the D&I of NMT programmes in a youth team sport. The specific objectives of this systematic review were to: (1) describe the characteristics of identified D&I-related studies (studies with at least one D&I outcome directly or indirectly assessed as primary, secondary or tertiary outcome); (2) evaluate factors associated with the D&I of NMT warm-up programme across socioecological levels, including barriers and facilitators; (3) examine the effect of D&I strategies in delivering NMT warm-ups across multiple socioecological levels; and (4) examine the influence of D&I strategies on injury rates. Our protocol was registered in PROSPERO (CRD42021271734), and the review is reported in accordance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines ( supplemental appendix S1 ).
Supplemental material
Search strategy and data sources.
A comprehensive search was developed with a librarian (KAH) in MEDLINE, incorporating four main concepts: child/youth, injury prevention, implementation/compliance/adherence and sports. The author team reviewed the final search strategy which was then piloted against the known key studies to ensure that the search was capturing relevant studies. Finally, the MEDLINE search was translated to the other databases. Searches were conducted 25 August 2021 (updated 16–18 August 2022; 5 September 2023). Search strategies are available in Supplemental Appendix S2 . Studies were identified by searching seven databases: MEDLINE(R) and EPUB Ahead of Print, In-Process & Other Non-Indexed Citations and Daily, Embase, Cochrane Central Register of Controlled Trials, Cochrane database of Systematic Reviews (all Ovid); CINAHL Plus with Full Text, SPORTDiscus with Full Text (EBSCO) and ProQuest Dissertations & Thesis Global.
Study selection and eligibility
All database search results were uploaded and duplicates were removed in Covidence (Veritas Health Innovation, Melbourne, Australia). Records were independently reviewed by authors in pairs (DL/IJS, CV/JK, KV/DL), starting with a screening of 50 randomly selected citations to assess inter-rater agreement with a threshold set at 90%. Each pair of reviewers performed title/abstract screening and full-text screening independently, providing reasons for exclusion at full-text stage ( figure 1 ). Any disagreements for exclusion, where a consensus could not be reached within pairs, were resolved by a senior author (OBAO). A secondary evaluation of included manuscripts was performed by senior authors (OBAO and CAE) to ensure appropriate inclusion. Study inclusion criteria were: (1) Participation in a team sport (male and female); (2) a minimum of 70% of participants as a youth (<19 years) or coaches of these youth teams; (3) reported dissemination and/or implementation outcomes (eg, self-efficacy, adherence, intention); (4) reported D&I strategies related to NMT warm-up programmes (ie, NMT delivery strategies, where applicable eg, in RCTs). Exclusion criteria were: (1) Studies evaluating rehabilitation programmes, non-team-based or physical education programmes; (2) non-peer-reviewed; (3) not English. The screening process was reported using the PRISMA flow diagram. 39
- Download figure
- Open in new tab
- Download powerpoint
Study identification Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram.
Risk of bias
To assess the risk of bias, three sets of paired reviewers independently used the Downs & Black (D&B) quality assessment tool. 40 The tool consists of a 27-item checklist (total score/33). A third senior reviewer (OBAO or CAE or AMR) resolved any disagreements. The rating of evidence and strength of recommendations were assessed using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) guidelines. 41–43
Frameworks/models
The proportion of studies that used D&I research theories/frameworks/models, including behaviour change frameworks/models, was examined to identify commonly used frameworks/models.
Efficacy-effectiveness orientation in RCTs
We assessed the components of 12 RCTs using the Rating Included Trials on the Efficacy-Effectiveness Spectrum (RITES) tool, as adapted by Maddox et al 44 RITES scores RCTs in systematic reviews based on a continuum of efficacy-effectiveness across four domains: Participant characteristics, trial setting, flexibility of intervention(s) and clinical relevance of experimental and comparison intervention(s) ( online supplemental table S1 ). 45 We modified the Likert grading system to classify studies depending on whether their emphasis was more on efficacy or effectiveness or balanced for both. Given that different aspects of each trial may fall in different places along the efficacy-effectiveness continuum, each RITES domain is scored independently and a composite score is not applicable. To minimise subjectivity, the RITES evaluation for included RCTs was completed by two reviewers (AMR and OBAO). Any disagreements were resolved through discussion to reach a consensus.
Study typologies and assessment of study relevance to D&I
The level of relevance of individual studies (RCTs and quasi-experiments) to D&I was determined based on the implementation-effectiveness hybrid taxonomy: Type 1 (primarily focused on clinical/intervention outcomes), Type 2 (balance focused on both clinical/intervention outcomes and D&I outcomes) and Type 3 (primarily or ‘fully’ (our adaptation) focused on D&I outcomes) studies. 36 46 For ease of interpretation of results, studies were rated considering three broad traditional research design categories (ie, hierarchy of evidence): RCTs, quasi-experimental and observational studies, including cohort, cross-sectional, pre-experimental, qualitative, mixed-methods and ecological studies. Observational studies were categorised as ‘fully focused’ observational-implementation (if only D&I outcomes were evaluated) or ‘partially focused’ observational-implementation (if a combination of clinical and D&I outcomes were evaluated’ D&I studies. 47 RCTs and quasi-experimental studies with Type 2 or Type 3 hybrid approaches were indicated as ‘highly relevant’ towards informing D&I best practices. Furthermore, observational-implementation studies that are fully focused on D&I were also indicated as ‘highly relevant’.
Data extraction
The extracted data included: study design, author, journal, year, population (eg, 13–17 years old female soccer players), participant demographics, D&I intervention strategies (eg, workshops, supplementary resources), D&I framework/model, control group strategies, D&I outcomes (eg, adoption, adherence, intention, fidelity, self-efficacy) and injury outcomes. Study design classification was completed based on data extracted and the process taken by authors, 48 which may have differed from the original classification. Furthermore, prospective, and retrospective cohort studies were consolidated into ‘cohort’ to improve ease of readability. D&I outcomes indicated as compliance were included in the appropriate adherence category as defined in Owoeye et al and described as ‘adherence-related’ outcomes, to maintain unified language across results; the full list is provided in online supplemental table S2 . 36 49–51 Based on the dose-response thresholds reported for NMT programmes within current literature, measures of adherence were used to indicate potential D&I effect ( online supplemental table S5 ). 24 36 52–54 Studies with cumulative utilisation (sessions completed/total possible) of ≥70%, utilisation frequency of ≥1.5 sessions/week or a significant association between D&I exposures and outcomes were defined as moderate-to-highly relevant and identified as having a potential D&I effect (ie, yes). Studies presenting cumulative utilisation <70%, utilisation frequency <1.5 sessions/week or no association between D&I exposures and outcomes were defined as low-to-no relevance (ie, no). Studies reporting both frequency utilisation and cumulative utilisation must both reach the established dose-response thresholds to be considered as having a potential D&I effect. D&I barriers and facilitators, factors influencing injury prevention implementation success and the identification of any frameworks used were also extracted and categorised into themes. Measures of potential effect for these results were summarised using OR, proportions and mean differences in D&I outcomes (eg, adoption, adherence). Injury-specific results were reported as incidence rate ratios, risk ratios, ORs or prevalence. D&I strategies were classified into various categories, including workshops, supplementary resources, personnel support, supervision and combinations of these strategies.
Equity, diversity and inclusion statement
Our author team is comprised of student and senior researchers across various disciplines with representation from low-to-middle-income countries. A variety of demographic, socioeconomic and cultural backgrounds were included in our study populations.
PRISMA flow, characteristics of included studies and risk of bias assessment
A total of 68 relevant studies were included from our initial and updated search yield of 9021 studies ( figure 1 ). Across included studies, 13 included only male youth participants, 13 included only female youth participants, 26 included both and 16 reported coach-focused findings. Sports represented were soccer (n=33), rugby (n=8), basketball (n=7), multisport (n=7), handball (n=5), floorball (n=3), field hockey (n=3), volleyball (n=1) and futsal (n=1).
Details of study characteristics and risk of bias are presented in online supplemental table S3 . D&B scores ranged from 4/33 to 24/33 (median=14/33) from a variety of study designs, including 20 RCTs, 16 cross-sectional, 9 quasi-experimental, 8 cohort, 6 qualitative, 3 ecological, 3 mixed-methods and 3 pre-experimental. The D&B scores for the two top D&I-related relevant studies—an RCT Type 2 study (n=1) was 21/33 and an RCT Type 3 hybrid study (n=1) was 17/33. Using the GRADE guidelines for the process of rating the quality of evidence available and interpreting the quality assessment, the strength of recommendations was ‘low’ given the multiplicity of designs. 42 43
Characteristics of current D&I-related studies
23 studies (33.8%) reported using a D&I /behaviour change framework/model. D&I frameworks included Reach, Effectiveness, Adoption, Implementation and Maintentance (RE-AIM) Framework (n=7), Consolidation Framework for Implementation Research (n=1), Precede-Proceed Model (n=1), Translating Research into Injury Prevention Practice (n=1) and Promoting Action on Research Implementation of Health Sciences (n=1) and the Adherence Optimisation Framework (n=1). Behaviour change models included the Health Action Process Approach (HAPA) (n=8), Theory of Planned Behaviour (n=1) and the Health Belief Model (n=1).
Assessment of study relevance to D&I
Two RCTs of 68 included D&I-related studies (2.9%) were identified as highly relevant to D&I best practices (ie, Type 2 or 3 hybrid approach). 55 56 18 (27.9%) RCTs reported a secondary analysis of D&I strategies 12 16 19 30 53 57–69 ; classified as Type 1 hybrids. Five (8.3%) quasi-experimental studies used Type 2 or Type 3 hybrid approach 22 70–73 ; the remaining studies (n=4; 5%) were classified as quasi-experimental Type 1 hybrids. 74–77 Many observational studies (n=17; 26.7%), 78–94 were highly relevant based on being fully-focused observational-implementation studies; 5 (6.7%) were partially-focused observational-implementation studies. 52 95–98 The remaining observational studies (n=17; 23.3%) were observational-implementation studies, 35 99–114 reporting D&I outcomes from a qualitative lens using interviews and surveys.
The RITES scores for the 14 D&I-related RCTs that examined injuries as primary outcome and D&I outcomes as secondary (Type 1 hybrid approach) are presented in table 1 . Almost all (13 of 14; 92.9%) of the RCTs focused mainly on intervention efficacy (as opposed to effectiveness) regarding the flexibility of NMT warm-up programmes. Cumulatively, effectiveness was rarely (7.1%) prioritised as a primary focus across all the 56 possible ratings of the RITES domains for all 14 studies. 50% of the domain ratings demonstrated efficacy as a priority and 42.9% of the ratings were indicated for a balance between efficacy and effectiveness.
- View inline
RITES domain scores for included trials
Contextual predictors of NMT warm-up programme implementation
50 (73.5% of total) studies identified ≥1 barrier or facilitator within their findings, with 10 (14.7% of total) specifically examining barriers/facilitators as their main objectives. Full list is provided in online supplemental table S4 . The most common barriers identified were time restrictions (n=30), 30 35 59 62 69 70 73 74 78 79 81 82 84 87–91 93 96 98 101 102 105 107 108 112 114 reduced buy-in/support (n=8) 62 75 84 87 105 110–112 and limited awareness of preventative effects of programmes (n=8). 74 84 103 104 107 109 113 Facilitators included comprehensive workshops from trained instructors (n=11), 53 71 78–80 84 90 96 99 100 112 accessibility of supplementary resources (n=10) 82 84 87 89 90 105 114 and uptake/support from multiple stakeholders (n=7). 56 67 84 101 103 105 112 Moreover, suggestions from multiple socioecological levels indicated that increasing programme education and support, increased sport-specific activities and improved awareness of preventive effects, influence NMT implementation success. 36 88 89 115 116 Figure 2 , adapted from Basow et al 117 illustrates the contextual factors reported in the literature. 117 This evidence-informed model shows the important barriers and facilitators that influence the end-user implementation of NMT warm-up programmes across the three key socioecological levels of change.
Contextual predictors of NMT implementation across multiple socioecological levels. (Adapted from Basow et al (2021)).(116). Notes. SE, self-efficacy. NMT, neuromuscular training. Bold represents top barrier(s)/facilitator(s).
51 (75%) studies used implementation strategies for NMT warm-up programmes. The most frequently used strategies were Workshops with supplementary Resources (WR; n=24), followed by Workshops with supplementary Resources, plus in-season Personnel support (WRP; n=14). Three studies employed both WR and WRP strategies. Other methods for implementation included only workshops (n=9), only supplementary resources (n=4), supplementary resources and personnel support (n=2), workshops with personnel support (n=1) and supervision (n=1). Note, some studies are duplicated throughout the table when multiple D&I strategies are compared. 22 53 56 86
The key D&I concepts that were reported within the included studies were adherence or adherence-related (eg, self-efficacy, translation and perception). Specific outcomes within these concepts were further examined from the individual study results. We did not have enough evidence to present a meta-analysis of the effect of D&I strategies on D&I outcomes. Therefore, online supplemental table S5 presents a qualitative summary of the relationships between reported D&I exposure and D&I outcomes. 40 studies reported adherence-related outcomes, of which 32 (80%) were indicated to have potential D&I effect. Studies using WRP (n=14) reported completing between 1.4 and 2.6 sessions/week and cumulative utilisation of 39–85.6%; 9 of these 14 studies have potential D&I effect. Studies using WR (n=24) presented utilisation frequency ranging from 0.8 to 3.2 sessions/week and cumulative utilisation of 55–98% of sessions; 16 of these 24 have potential D&I effect. In studies evaluating workshops only (n=9; 22%), frequency utilisation was reported between 1 and 2 sessions/week across eight of the nine studies and one study had 52% cumulative utilisation; two have potential D&I effect.
Effects of D&I strategies on injury outcomes
Three RCTs specifically examined the effects of the D&I strategies used to deliver NMT programmes on injury outcomes ( table 2 ). Two studies that compared both WR and WRP to supplementary resource only found no significant differences between strategies, 53 56 they reported reduced injury rates in the highest adherence groups by 56% and 72%, respectively. Another study comparing WR and WRP to a standard of practice warm-up found a 36% reduction of ankle and knee injuries when using WR and a 38% reduction in ankle and knee injuries without supervision. 22 There were no significant differences in injury rates between groups.
Injury Outcomes by D&I strategies and adherence
This study evaluated current literature to inform evidence-based best practices for the D&I of NMT programmes in youth team sport. To our knowledge, this is the first systematic review evaluating the D&I of NMT programmes in youth sport. To improve the practical implementation of NMT warm-ups, factors associated with implementation success and current best practices for delivering context-specific NMT programmes are required to be evaluated. 118 In this review, we found few D&I-related studies use D&I or behaviour change frameworks, theories or models to guide their research questions. We discovered the number of RCTs examining the effectiveness of D&I strategies for NMT programme delivery is limited. Common barriers to NMT implementation include programme flexibility and time restrictions; and the use of coach workshops and supplementary resources are currently the primary strategy in NMT programme D&I facilitation.
One-third of the included studies used a D&I framework or behaviour change model in their research work. The HAPA and RE-AIM models were the most frequently used. These models are a conceptual and organised combination of theories required to direct the design, evaluation and translation of evidence-based interventions (NMT programmes) and the context in which they are being implemented. 36 71 119 It is imperative for D&I studies to use these frameworks/models to fully understand specific implementation processes and contexts. Future D&I studies should consider using appropriate frameworks or models, including adaptations and combination of models to guide their specific aims.
Relevance to D&I
Across the relevant literature, a variety of designs and levels of evidence were included.
Of 68 studies, 7 (10.3%) were found to be ‘highly relevant’ toward informing D&I best practice (2 (2.9%) RCTs, 5 (7.4%) quasi-experimental). Other ‘relevant’ studies evaluated implementation as secondary objectives (Type 1 hybrid designs) and/or were of lower level of evidence. 33 observational studies were ‘highly relevant’ to D&I, assessing D&I outcomes and barriers and facilitators from a qualitative lens. While these studies are important for understanding D&I context, more high-quality and highly relevant studies such as RCTs and quasi-experimental designs using the Type 3 hybrid approach, or non-hybrid approach focused on solely evaluating the effectiveness of D&I strategies, are needed to advance the widespread adoption and continued use of NMT programmes in youth team sport.
Effectiveness versus efficacy
Effectiveness is indicative of an evidence-informed intervention’s readiness for practical implementation. 36 Findings from our RITES scores evaluation indicate that the majority of the RCTs had a primary focus on efficacy and not effectiveness. Although many RCT studies had a fair balance between efficacy and effectiveness for participant characteristics, trial settings and clinical relevance domains (≥50% of RCTs), there is a lack of flexibility in the development and evaluation of the evidence supporting current NMT warm-up programmes. These disparities regarding practical implementation have implications for D&I research and practice in this field. Current NMT programmes may need to be modified or adapted to the local context and evaluated further to improve implementation in youth sport settings.
Contextual considerations
In our Adapted Socioecological Model ( figure 2 ), we demonstrate that the utilisation of NMT programmes by individual players within youth team sport can depend on their coach adopting and implementing the warm-up, which may also be dependent on larger organisational systems. Barriers related to end-users’ success in wide-spread adoption and long-term maintenance can be moderated; however, researchers and implementers have to be intentional about tackling these recognised barriers and associated challenges 25 87 104 115 ; integrating the facilitators of successful implementation intending to reduce and address these obstacles is essential. The barriers and facilitators identified in this systematic review provide insight into the combination of D&I strategies that should be formulated and tested by D&I researchers in the sports injury prevention field.
Within the current review, lack of time, whether it be learning, instructing and/or practicing the programme, is a common barrier that plays a significant role in implementation. A recent narrative review focused solely on the barriers and facilitators associated with exercise-based warm-up programmes showed similar conclusions regarding time restrictions. 115 Collective themes within this literature for players, coaches and organisations found that reduced buy-in and support at different levels impacted the adoption of NMT warm-up programmes. The lack of awareness and knowledge of the injury prevention benefits of NMT warm-up programmes also presented major barriers to buy-in, leading to reduced implementation success. Future interventions should ensure that education about evidence-informed injury prevention outcomes associated with programme adherence is integrated within their D&I strategies.
D&I science is a growing field of study. A variety of D&I outcomes were identified such as self-efficacy, intention, reach, outcome expectancy and most commonly, adherence or adherence-related outcomes. These outcomes were evaluated using different D&I strategies for NMT warm-up programmes. The most commonly reported strategies were Workshops with supplementary Resources with/without in-season Personnel support. Evaluation of D&I outcomes showed that adherence or adherence-related outcomes were most frequently reported across studies. Various measures of adherence as defined by Owoeye et al (2020) were identified, including cumulative utilisation, utilisation frequency, utilisation fidelity, duration fidelity and exercise fidelity. 36
Adherence remains the most common D&I outcome in the sport injury prevention literature. 36 120 In this review, we defined adherence and adherence-related thresholds for a moderate-to-high dose-response to be ≥70% cumulative utilisation and/or ≥1.5 session/week to achieve the desired protective effects. This was done with consideration of pragmatism and a practical balance between programme efficacy and effectiveness given the existing literature. 24 91 32 of 40 studies (80%) from those with adherence or adherence-related outcomes had a potential D&I effect based on a moderate-to-high adherence or adherence-related outcome level. The use of WR and WRP was the most common D&I strategies for delivering NMT warm-up programmes. While there are several areas for improvement for the practical D&I of NMT warm-up programmes in youth sport settings, the use of comprehensive workshops and supplementary resources at various levels, particularly with coaches, appears to be the optimal best practice. However, only two ‘highly relevant’ D&I studies (RCTs) from the current systematic review presented conclusions based on the effectiveness of D&I strategies and outcomes specifically.
Many studies (n=26/68; 38.2%) included both male and female participants; however, no sex-differences were described. When examining D&I outcomes, only 7/26 (26.9%) had moderate-to-high adherence when looking at both male and female youth players. In total, 84.6% of the female-only (11/13) and 72.7% of the male-only studies (8/11) reported moderate-to-high adherence levels. These findings suggest greater attention and efforts for adherence and implementation of NMT programmes in the male youth team sport setting may need further consideration compared with the female youth sport context.
Of the preliminary evidence for Type 2 and 3 hybrid designs, the literature highlighted in the synthesis of this data that WR are effective strategies in injury prevention and showed more moderate-to-high adherence levels. Given that most studies are doing some form of WR, adding in-season personnel support does not increase the protective effect and may be less sustainable given that resources, time and support are significant barriers to the D&I of these programmes.
Additionally, greater implementation and programme buy-in were found in studies where uptake of these NMT programmes was supported across multiple stakeholders, particularly at the organisation level. 19 67 90 103 112 Catering to programme deliverers (coaches, organisations, parents) and evaluating their awareness, perception and self-efficacy may help further inform our understanding of D&I and how we can best work to promote programme uptake further.
D&I strategies and injury outcomes
The findings from this systematic review suggest that while various D&I intervention strategies are effective at reducing injuries in youth team sports, the ranges of injury rate ratios are similar across studies employing different strategies (32–88% lower injury rates across WR strategy studies and 41–77% lower injury rates across WRP strategy studies). 22 53 56 Although this was not the proposed evaluation of these studies, our findings demonstrate that the use of workshops may influence D&I success and the availability of supplementary resources alone may not be efficacious. Future evaluation of the influence of delivery strategies should be considered.
Future directions
Using facilitators to reduce barrier burden.
Regarding NMT strategy evaluation, our findings show that most of the current programmes focus on efficacy over effectiveness, particularly in the aspect of intervention flexibility; this suggests a need for the adaptation of NMT programmes to fit local contexts. NMT programme developers should consider more enjoyable and user-friendly exercises that include sport-specific activities (eg, ball work, partner drills, tags). Increasing variations also improves player buy-in and increases intrinsic motivation. At a coaching level, workshops on NMT programmes should include evidence-informed education on the injury prevention benefits and should incorporate content addressing coach self-efficacy to enhance implementation quality. 16 100 121 An ongoing pragmatic evaluation of NMT programme effectiveness is warranted as they undergo adaptation to local contexts.
Organisations have expressed limited knowledge and education for implementation as a significant barrier to successful NMT programme use. 90 99 101 105 112 115 122 Implementers should look to provide accessible resources and encourage further support from multiple stakeholders, including the governing bodies. This could lead to policy changes within the club and result in greater uptake of these programmes long-term. Collaborations among stakeholders (researchers, youth sport administrators, coaches and players) in programme development, evaluation, D&I are necessary to improve efforts for impactful practical translation of programmes.
Research recommendations
The support for NMT programmes within youth sport is extensive. 28 Although these programmes have been shown to be effective for injury prevention in many sports, 10 11 sport representation across D&I studies in our review was limited. Scaling up of NMT programmes and supporting continued research into other sports is vital for increased context-specific D&I of these programmes to reduce the overall burden of youth sport injuries.
Compliance and adherence were often used interchangeably, despite having distinct definitions. Although their mathematical calculations are similar, these two constructs are contextually different. Compliance refers to individuals conforming to prescribed recommendations in controlled intervention settings, 123 while adherence refers to the agreement of an individual’s behaviour to recommended evidence-based interventions in uncontrolled settings. 36 Standardised definitions should be considered more frequently by researchers to build on current knowledge and inform future D&I research.
Using D&I frameworks/models can improve NMT programme implementation success in a practical setting. 71 124 Application of D&I frameworks/models, including behaviour change models, 124 is limited in injury prevention and this is reflected in the current systematic review. Future studies should use D&I frameworks/models to help guide the implementation of these NMT programmes. In doing so, researchers can gain a better understanding of the contextual and behaviour change aspects related to youth sport injury prevention. 115
Limitations
Given the broad nature of our research question, specific results were required for inclusion. Despite being specific to our objectives, our limitations set for participant age range, team sport settings and English language studies only, may have resulted in missing other studies that evaluated D&I interventions and outcomes related to NMT programmes.
Due to the heterogeneous nature of studies, meta-analysis was not possible for any of our objectives. Inclusion of various study designs, although comprehensive, impeded this process and resulted in inconsistent injury and adherence definitions across our population of interest. Furthermore, the subjective nature of many qualitative studies included may have resulted in variability within the data extracted. With the varied definitions used for each specific outcome and design, we looked to consolidate the terminology used into more succinct and unified language and we encourage this to be employed by researchers.
Methodological flaws existed in the included studies that may warrant caution about the interpretation of our conclusions. For example, many of the included studies did not include power calculations or reported low power, increasing the chance of Type 2 error. Further, many studies did not consider confounding or effect modification in their analyses or failed to report the validity of measurement tools used for injury data collection. We also acknowledge that publication bias may have favoured the inclusion of studies demonstrating significant findings (eg, effectiveness, efficacy). By considering quality assessment as an objective, we aimed to account for these limitations.
There was limited evidence supporting the effect of D&I strategies on D&I-specific outcomes. There were only two high-level evidence (RCTs) studies in this review that directly discussed the matter of D&I strategies on D&I outcomes. 55 56 D&I-related outcomes were evaluated as secondary objectives in other high-level evidence studies, therefore, we could only examine the relationship between D&I strategy and outcome to assess if the strategy used resulted in moderate-to-high adherence levels, given our pre-established thresholds.
Conclusions
This systematic review demonstrates that: (1) Few D&I-related studies are based on D&I or behaviour change theories, frameworks or models; (2) few RCTs have examined the effectiveness of D&I strategies for delivering NMT programmes; (3) programme flexibility and time restrictions are the most common barriers to implementation and; (4) a combination of coach workshops and supplementary resources are currently the primary strategy facilitating NMT programme D&I; however their effectiveness is only evaluated in a few studies. This systematic review provides foundational evidence to facilitate evidence-informed knowledge translation practices in youth sport injury prevention. Transitioning to more high-quality D&I research RCTs and quasi-experimental designs that leverage current knowledge of barriers and facilitators, incorporates Type 2 or Type 3 hybrid approaches and uses behaviour change frameworks are important next steps to optimise the translation of NMT programmes into routine practice in youth team sport settings.
Ethics statements
Patient consent for publication.
Not applicable.
Ethics approval
- Cumming SP ,
- Australian Sports Commission
- Meeuwisse DW ,
- Eliason PH , et al
- Child and Adolescent Health Measurement Initiative
- Emmonds S ,
- Weaving D ,
- Lara-Bercial S , et al
- Merkel DL ,
- Raysmith BP ,
- Charlton PC
- Brunner R ,
- Friesenbichler B ,
- Casartelli NC , et al
- Whittaker JL , et al
- Meeuwisse WH
- Gianotti S ,
- Jacquet C ,
- Verhagen E , et al
- Marshall DA ,
- Lopatina E ,
- Lacny S , et al
- Owoeye OBA ,
- Akinbo SRA ,
- Tella BA , et al
- Palacios-Derflingher LM ,
- Pasanen K ,
- Parkkari J ,
- Pasanen M , et al
- Soligard T ,
- Myklebust G ,
- Steffen K , et al
- Thorborg K ,
- Krommes KK ,
- Esteve E , et al
- Webster KE ,
- Räisänen AM , et al
- Räisänen AM ,
- van den Berg C ,
- Owoeye OBA , et al
- Pfeifer K , et al
- Richmond SA ,
- Doyle-Baker PK , et al
- Barengo N ,
- Meneses-Echávez J ,
- Ramírez-Vélez R , et al
- Bizzini M ,
- Sadigursky D ,
- De Lira DNL , et al
- Åkerlund I ,
- Sonesson S , et al
- Hislop MD ,
- Stokes KA ,
- Williams S , et al
- Hopper AJ ,
- Joyce C , et al
- Bergeron MF ,
- Mountjoy M ,
- Armstrong N , et al
- De Ste Croix M ,
- Sanchez SH , et al
- Creech MJ ,
- Peterson DC , et al
- Rauvola RS ,
- Brownson RC
- Owoeye OB ,
- Olawale OA , et al
- Niederer D ,
- Vogt L , et al
- Ardern CL ,
- Büttner F ,
- Andrade R , et al
- Guyatt GH ,
- Vist GE , et al
- Kunz R , et al
- Siemieniuk R ,
- Maddox CD ,
- Subialka JA ,
- Young JL , et al
- Wieland LS ,
- Berman BM ,
- Altman DG , et al
- Landes SJ ,
- McBain SA ,
- Schwartz S ,
- Duncan DT , et al
- Ranganathan P
- Proctor E ,
- Silmere H ,
- Raghavan R , et al
- Schwarzer R
- Hägglund M ,
- Atroshi I ,
- Wagner P , et al
- Steffen K ,
- Romiti M , et al
- Sugimoto D ,
- Barber Foss KD , et al
- Schneider B , et al
- Meeuwisse WH ,
- Al Attar WSA ,
- Alzahrani H , et al
- Alizadeh MH ,
- Shahrbanian S , et al
- Waldén M , et al
- Akasaka K ,
- Otsudo T , et al
- Leppänen M ,
- Vasankari T , et al
- LaBella CR ,
- Huxford MR ,
- Grissom J , et al
- Loppini M ,
- Berton A , et al
- Parsons JL ,
- Carswell J ,
- Nwoba IM , et al
- Rössler R ,
- Bizzini M , et al
- Slauterbeck JR ,
- Choquette R ,
- Tourville TW , et al
- Olsen OE , et al
- Mattacola CG ,
- Bush HM , et al
- Hancock MV ,
- Stokes KA , et al
- RÄisÄnen AM , et al
- Barboza SD ,
- Emery C , et al
- Hellquist E ,
- Ahlqvist K , et al
- Tomsovsky L ,
- Whatman C , et al
- Verhagen E ,
- Gouttebarge V , et al
- Celebrini RG ,
- Miller WC , et al
- Franchina M ,
- Tercier S , et al
- Register-Mihalik J ,
- Choquette R , et al
- Lindblom H ,
- Carlfjord S ,
- Ljunggren G ,
- Perera NKP ,
- Merrett CK ,
- Linnéll J , et al
- Myklebust G , et al
- O’Brien J ,
- Santner E ,
- Befus K , et al
- Räisänen A ,
- Black AM , et al
- Sonesson S ,
- Lindblom H , et al
- Nilstad A ,
- Thein-Nissenbaum J ,
- Ageberg E ,
- Lucander K , et al
- Brodin EM ,
- Watkins R ,
- Cornelissen MH ,
- Baan A , et al
- Donaldson A ,
- Callaghan A ,
- Taylor JR ,
- Novak MA , et al
- MacFarlane AJ ,
- Weiss-Laxer NS , et al
- McGuine TA ,
- Pennuto A , et al
- Munoz-Plaza C ,
- Davis A , et al
- Norcross MF ,
- Johnson ST ,
- Bovbjerg VE , et al
- Jimenez P ,
- Oliver JL , et al
- Denegar CR , et al
- Lambert M , et al
- Withall AL , et al
- Minnig MC ,
- Hawkinson L ,
- Root HJ , et al
- Macpherson A , et al
- Fenelon D , et al
- Bruinsma A , et al
- Verhagen EALM , et al
- Brown JC , et al
- Bogardus RL ,
- Martin RJ ,
- Richman AR , et al
Supplementary materials
Supplementary data.
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1
- Data supplement 2
X @carlavdb_, @amraisanen, @KatiPasanen, @Kat_Schneider7, @CarolynAEmery, @owoeye_oba
Contributors DL, CE and OBAO contributed to development of study proposal and design. DL, CvdB, AMR, IJS, KV, JK, AH, CE and OBAO conducted search, study selection and screening, data extraction and synthesis and quality assessment. DL led the writing of the manuscript and was the guarantor for the project. All authors contributed to drafting and revising the final manuscript. All authors approved the submitted version of the manuscript.
Funding This study was funded by Canadian Institutes for Health Research Foundation Grant Program (PI CAE).
Competing interests OBAO is a Deputy Editor for the British Journal of Sports Medicine. CE, KJS and KP are Associate Editors for the British Journal of Sports Medicine.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
Read the full text or download the PDF:
IMAGES
VIDEO
COMMENTS
Examples of literature reviews. Step 1 - Search for relevant literature. Step 2 - Evaluate and select sources. Step 3 - Identify themes, debates, and gaps. Step 4 - Outline your literature review's structure. Step 5 - Write your literature review.
Steps for Conducting a Lit Review; Finding "The Literature" Organizing/Writing; APA Style This link opens in a new window; Chicago: Notes Bibliography This link opens in a new window; MLA Style This link opens in a new window; Sample Literature Reviews. Sample Lit Reviews from Communication Arts; Have an exemplary literature review? Get Help!
A literature review is a critical analysis and synthesis of existing research on a particular topic. It provides an overview of the current state of knowledge, identifies gaps, and highlights key findings in the literature. 1 The purpose of a literature review is to situate your own research within the context of existing scholarship ...
A literature review is a document or section of a document that collects key sources on a topic and discusses those sources in conversation with each other (also called synthesis ). The lit review is an important genre in many disciplines, not just literature (i.e., the study of works of literature such as novels and plays).
Literature Review Guide: Examples of Literature Reviews. How to create Literature reviews ... Emerald Infographic; Top Tip. All good quality journal articles will include a small Literature Review after the Introduction paragraph. ... Non-verbal communication between nurses and people with an intellectual disability: A review of the literature ...
1. Outline and identify the purpose of a literature review. As a first step on how to write a literature review, you must know what the research question or topic is and what shape you want your literature review to take. Ensure you understand the research topic inside out, or else seek clarifications.
Writing a literature review requires a range of skills to gather, sort, evaluate and summarise peer-reviewed published data into a relevant and informative unbiased narrative. Digital access to research papers, academic texts, review articles, reference databases and public data sets are all sources of information that are available to enrich ...
This article is organized as follows: The next section presents the methodology adopted by this research, followed by a section that discusses the typology of literature reviews and provides empirical examples; the subsequent section summarizes the process of literature review; and the last section concludes the paper with suggestions on how to improve the quality and rigor of literature ...
A literature review is a survey of scholarly sources on a specific topic. It provides an overview of current knowledge, allowing you to identify relevant theories, methods, and gaps in the existing research. There are five key steps to writing a literature review: Search for relevant literature. Evaluate sources. Identify themes, debates and gaps.
The best proposals are timely and clearly explain why readers should pay attention to the proposed topic. It is not enough for a review to be a summary of the latest growth in the literature: the ...
As mentioned above, writing your literature review is a process, which I'll break down into three steps: Finding the most suitable literature. Understanding, distilling and organising the literature. Planning and writing up your literature review chapter. Importantly, you must complete steps one and two before you start writing up your chapter.
We start off by discussing the five core sections of a literature review chapter by unpacking our free literature review template. This includes: The literature review opening/ introduction section. The theoretical framework (or foundation of theory) The empirical research. The research gap.
When writing a literature review it is important to start with a brief introduction, followed by the text broken up into subsections and conclude with a summary to bring everything together. A summary table including title, author, publication date and key findings is a useful feature to present in your review (see Table 1 for an example).
2. MOTIVATE YOUR RESEARCH in addition to providing useful information about your topic, your literature review must tell a story about how your project relates to existing literature. popular literature review narratives include: ¡ plugging a gap / filling a hole within an incomplete literature ¡ building a bridge between two "siloed" literatures, putting literatures "in conversation"
As mentioned previously, there are a number of existing guidelines for literature reviews. Depending on the methodology needed to achieve the purpose of the review, all types can be helpful and appropriate to reach a specific goal (for examples, please see Table 1).These approaches can be qualitative, quantitative, or have a mixed design depending on the phase of the review.
Literature reviews are in great demand in most scientific fields. Their need stems from the ever-increasing output of scientific publications .For example, compared to 1991, in 2008 three, eight, and forty times more papers were indexed in Web of Science on malaria, obesity, and biodiversity, respectively .Given such mountains of papers, scientists cannot be expected to examine in detail every ...
15 Literature Review Examples. By Chris Drew (PhD) / December 6, 2023. Literature reviews are a necessary step in a research process and often required when writing your research proposal. They involve gathering, analyzing, and evaluating existing knowledge about a topic in order to find gaps in the literature where future studies will be needed.
These sections serve to establish a scholarly basis for the research or discussion within the paper. In a standard 8000-word journal article, the literature review section typically spans between 750 and 1250 words. The first few sentences or the first paragraph within this section often serve as an introduction.
A literature review is a surveys scholarly articles, books and other sources relevant to a particular. issue, area of research, or theory, and by so doing, providing a description, summary, and ...
Level allow 1 headings readers introduce to clearly. a new indicate thought, a new idea, section argument, within or the topic. review. Level 1 headings Each are helpful Level 1 Subheading should be because they allow readers flushed left on the page. to and clearly formatted indicate a in new ALL-.
A literature review is a compilation of current knowledge on a particular topic derived from the critical evaluation of different scholarly sources such as books, articles, and publications, which is then presented in an organized manner to relate to a specific research problem being investigated. It highlights the methods, relevant theories, and gaps in existing research on a particular ...
Examples of Literature Reviews in Journal Articles and Disserations. The stigma of childhood obesity: A literature review by Janel Swaye MacDermott. Journal Articles. Papastergiou, Marina. 2009. "Exploring the potential of computer and video games for health and physical education: A literature review." Computers & Education 53, no. 3: 603-622.
A thematic literature review serves as a critical tool for synthesizing research findings within a specific subject area. By categorizing existing literature into themes, this method offers a structured approach to identify and analyze patterns and trends across studies. The primary goal is to provide a clear and concise overview that aids ...
Amiodarone-induced thyroid dysfunction (AIT) is a side-effect associated with the use of Amiodarone for the treatment of refractory arrythmias. Resulting hyperthyroidism can precipitate cardiac complications, including cardiac ischemia and myocardial infarction, although this has only been described in a few case reports. We present here a clinical scenario involving a 66-year-old male ...
Literature review. The review of previous TTs from SKR and the literature search using PubMed, Cinahl and Medline revealed 32 triggers (refer to supplement 1 and 2).The structure of the ATT was constructed to be the same as that of previous TTs from SKR, and each of the 32 triggers was defined and received definition for the trigger to be positive.
This article is a practical guide to conducting data analysis in general literature reviews. The general literature review is a synthesis and analysis of published research on a relevant clinical issue, and is a common format for academic theses at the bachelor's and master's levels in nursing, physiotherapy, occupational therapy, public health and other related fields.
Calcitonin gene-related peptide (CGRP) is the most promising candidate to become the first migraine biomarker. However, literature shows clashing results and suggests a methodological source for such discrepancies. We aimed to investigate some of these methodological factors to evaluate the actual role of CGRP as biomarker. Previous to the experimental part, we performed a literature review of ...
It may also explain why, despite patient reports and legal findings of harm, the scholarly literature tends to endorse pelvic mesh as effective and safe. In 2009, the International Committee of Medical Journal Editors (ICMJE) introduced requirements for detailed disclosure of all relevant COI by any author . All articles in this review were ...
Objective To evaluate best practices for neuromuscular training (NMT) injury prevention warm-up programme dissemination and implementation (D&I) in youth team sports, including characteristics, contextual predictors and D&I strategy effectiveness. Design Systematic review. Data sources Seven databases were searched. Eligibility The literature search followed Preferred Reporting Items for ...
International Journal of Fashion Design, ... a content analysis systematic literature review. Kristian Hogans a Department of Family and Consumer Sciences, Alabama A&M University, Huntsville, ... This study aimed to assess the skill and knowledge areas emphasised in a sample of US-based undergraduate apparel merchandising programs, as well as ...