- Search Menu
- Themed Collections
- Editor's Choice
- Ilona Kickbusch Award
- Supplements
- Author Guidelines
- Submission Online
- Open Access Option
- Self-Archiving Policy
- About Health Promotion International
- Editorial Board
- Advertising and Corporate Services
- Journals on Oxford Academic
- Books on Oxford Academic


Article Contents
Introduction, authors' contributions, acknowledgements.
- < Previous
Nurses' roles in health promotion practice: an integrative review
- Article contents
- Figures & tables
- Supplementary Data
Virpi Kemppainen, Kerttu Tossavainen, Hannele Turunen, Nurses' roles in health promotion practice: an integrative review, Health Promotion International , Volume 28, Issue 4, December 2013, Pages 490–501, https://doi.org/10.1093/heapro/das034
- Permissions Icon Permissions
Nurses play an important role in promoting public health. Traditionally, the focus of health promotion by nurses has been on disease prevention and changing the behaviour of individuals with respect to their health. However, their role as promoters of health is more complex, since they have multi-disciplinary knowledge and experience of health promotion in their nursing practice. This paper presents an integrative review aimed at examining the findings of existing research studies (1998–2011) of health promotion practice by nurses. Systematic computer searches were conducted of the Cochrane databases, Cinahl, PubMed, Web of Science, PsycINFO and Scopus databases, covering the period January 1998 to December 2011. Data were analysed and the results are presented using the concept map method of Novak and Gowin. The review found information on the theoretical basis of health promotion practice by nurses, the range of their expertise, health promotion competencies and the organizational culture associated with health promotion practice. Nurses consider health promotion important but a number of obstacles associated with organizational culture prevent effective delivery.
The role of nurses has included clinical nursing practices, consultation, follow-up treatment, patient education and illness prevention. This has improved the availability of health-care services, reduced symptoms of chronic diseases, increased cost-effectiveness and enhanced customers' experiences of health-care services ( Strömberg et al ., 2003 ; Griffiths et al ., 2007 ). In addition, health promotion by nurses can lead to many positive health outcomes including adherence, quality of life, patients' knowledge of their illness and self-management ( Bosch-Capblanc et al ., 2009 ; Keleher et al ., 2009 ). However, because of the broad field of health promotion, more research is needed to examine the role of health promotion in nursing ( Whitehead, 2011 ).
The concept of health promotion was developed to emphasize the community-based practice of health promotion, community participation and health promotion practice based on social and health policies ( Baisch, 2009 ). However, empirical studies indicate that nurses have adopted an individualistic approach and a behaviour-changing perspective, and it seems that the development of the health promotion concept has not influenced practical health promotion practices by nurses ( Casey, 2007a ; Irvine, 2007 ). On the other hand, there has been much discussion about how to include health promotion in nursing programmes and how to redirect nurse education from being disease-orientated towards a health promotion ideology ( Rush, 1997 ; Whitehead, 2003 ; Mcilfatrick, 2004 ).
The aim of this integrative review was to collate the findings of past research studies (1998–2011) of nurses' health promotion activities. The research questions addressed were: (i) What type of health promotion provides the theoretical basis for nurses' health promotion practice? (ii) What type of health promotion expertise do nurses have? (iii) What type of professional knowledge and skills do nurses undertaking health promotion exhibit? (iv) What factors contribute to nurses' ability to carry out health promotion?
An integrative review was chosen because it allowed the inclusion of studies with diverse methodologies (for example, qualitative and quantitative research) in the same review ( Cooper, 1989 ; Whittemore, 2005 ; Whittemore and Knafl, 2005 ). Integrative reviews have the potential to generate a comprehensive understanding, based on separate research findings, of problems related to health care ( Kirkevold, 1997 ; Whittemore and Knafl, 2005 ). The integrative review was split into the following phases: problem identification, literature search, data evaluation, data analysis and presentation of the results ( Whittemore and Knafl, 2005 ).
Search method
Several different databases were searched to identify relevant published material. Systematic searches of the Cochrane databases, Cinahl, PubMed, Web of Science, PsycINFO and Scopus databases were undertaken using the search string ‘nurs* AND professional competence* OR clinical competence* OR professional skill* OR professional knowledg* OR clinical skill* OR clinical knowledg* AND health promotion OR preventive health care OR preventive healthcare’. The searches were limited to studies published during the period 1998–2011 because, prior to 1998, nurses' health promotion practice was mainly linked to health education.
Search result
The original search identified 1141 references: 119 in the Cochrane databases; 227 in Cinah, 345 in PubMed, 128 in the Web of Science, 100 in PsycINFO and 222 in Scopus. After duplicate papers were excluded one researcher (V.K.) read the titles and abstracts of the remaining 412 research papers. No specific evaluation criteria are employed when conducting an integrative review using diverse empirical sources; one approach is to evaluate methodological quality and informational value ( Whittemore and Knafl, 2005 ). All three researchers (V.K., K.T. and H.T.) defined the inclusion criteria together. Studies were included in the integrative review if they met the following criteria: the language had to be English, Swedish or Finnish, as translators for other languages were not available and the papers had to be published in peer-reviewed journals and describe nurses' health promotion roles, knowledge or skills and/or factors that contributed to nurses' ability to implement health promotion in nursing delivered through hospital or primary health-care services. The main exclusion criteria were: the published works were editorials, opinions, discussions or textbooks, or they described health promotion programmes, competencies other than health promotion or nursing curricula, or if the group studied included patients. The included studies were tabulated in chronological order under the following headings: citation, aim of the paper, methodology, size of the sample, measured variables, method of analysis, major results, concepts used as the basis of the study and limitations. Studies included in this review are available in Supplementary data, Table S1 .
Data analysis
Conducting an integrative review that analyses various types of research paper is a major challenge ( Whittemore and Knafl, 2005 ). In this review, the concept map method was adopted for both data analysis and presentation of the results. The use of concept mapping promotes conceptual understanding and provides a strategy for analysing and organizing information and identifying, graphically displaying and linking concepts. The concept map method was applied according to the recommendations of Novak and Gowin [( Novak and Gowin, 1984 ), p. 15–40] and Novak ( Novak, 1993 , 2002 , 2005 ). According to Novak ( Novak, 1993 , 2002 , 2005 ) the process of concept mapping involves six phases: (i) Identify a key question that focuses on a problem, issue or knowledge central to the purpose of the concept map. (ii) Identify concepts through the key question. (iii) Start to construct the concept map by placing the key concepts at the top of the hierarchy. After that, select defining concepts and arrange hierarchially below of the key concepts. (iv) Combine the concepts by cross-links or links between concepts in different segments or domains of the concept map. (v) Give the cross-links a name of a word or two. (vi) To concepts can be added specific examples of events or objectives that clarify the meaning of the concept.
All three researchers (V.K., K.T. and H.T.) were involved in the concept mapping process. The process proceeded as follows: first, one researcher (V.K.) read studies that met the inclusion criteria and the concepts were identified through the four research questions upon which the review is based. Second, one researcher (V.K.) began to construct four concept maps hierarchically. This was achieved by putting the key concepts on the top of the left side of a page then listing definitions of the concepts down the middle of each page. Other researchers (K.T. and H.T.) verified the first and the second phases of the concept mapping process. Third, one researcher (V.K.) continued the construction of each concept map by combining main concepts and definition concepts using links that were then named. Other researchers (K.T. and H.T.) critically evaluated the concept maps thus produced. Fourth, one researcher (V.K.) selected examples of the main concepts and these were listed on the right side of each page for clarification.
In the end 40 research papers, were included in our integrative review. The research papers were methodologically very diverse: 16 of them included qualitative approaches; 14 were different types of reviews; 8 were quantitative; 1 used concept analysis and 1 was a mixed-method study. Twelve empirical studies were conducted in hospitals and fourteen in primary health-care settings. Eleven studies were published in the period 1998–2004, twenty-two between 2005 and 2009 six between 2010 and 2011.
What type of health promotion provides the theoretical basis for nurses' health promotion practice?
The theoretical basis underlying nurses' health promotion activities was identified in 25 of the research papers ( Benson and Latter, 1998 ; McDonald, 1998 ; Robinson and Hill, 1998 ; Sheilds and Lindsey, 1998 ; Burge and Fair, 2003 ; Hopia et al ., 2004 ; Whitehead, 2004 , 2006a , b , c , 2009 , 2011 ; Berg et al ., 2005 ; Runciman et al ., 2006 ; Casey, 2007a , b ; Folke et al ., 2007 ; Irvine, 2007 ; Piper, 2008 ; Witt and Puntel de Almeida, 2008 ; Chambres and Thompson, 2009 ; Fagerström, 2009 ; Richard et al ., 2010 ; Samarasinghe et al ., 2010 ; Povlsen and Borup, 2011 ). According to these papers the theoretical basis of health promotion reflects the type of practical actions undertaken by nurses to promote the health of patients, families and communities. The research suggests that nurses work from either a holistic and patient-oriented theoretical basis or take a chronic diseases and medical-oriented approach. These theoretical foundations were considered to represent the main concepts of health promotion orientation and public health orientation in this review (Figure 1 ).
Concepts and examples of the theoretical basis of nurses' health promotion activities.
Health promotion orientation
The most common factor influencing the concept of health promotion orientation was individual perspective ( Robinson and Hill, 1998 ; Hopia et al ., 2004 ; Runciman et al ., 2006 ; Casey, 2007a ; Chambres and Thompson, 2009 ; Samarasinghe et al ., 2010 ; Povlsen and Borup, 2011 ). When nurses' health promotion activities were guided by individual perspective nurses' exhibited a holistic approach in their health promotion practice, they concentrated on activities such as helping individuals or families to make health decisions or supporting people in their engagement with health promotion activities ( Hopia et al ., 2004 ; Irvine, 2007 ; Chambres and Thompson, 2009 ; Samarasinghe et al ., 2010 ; Povlsen and Borup, 2011 ). Nurses' strategies for health promotion included giving information to patients and providing health education ( Casey, 2007a ). However, patient participation was mainly limited to personal aspects of care, such as letting patients decide on a menu, when to get out of bed and what clothes they wanted to wear ( Casey, 2007a ).
The second common defining concept of health promotion orientation was empowerment, which was related to collaboration with individuals, groups and communities ( McDonald, 1998 ; Berg et al., 2005 ; Whitehead, 2006a ; Irvine, 2007 ; Piper, 2008 ; Richard et al ., 2010 ; Samarasinghe et al ., 2010 ). Such orientation was described in these studies in terms of nurse–patient communication and patient, group and community participation. Although these studies found empowerment to be one of the most important theoretical bases for health promotion activities by nurses, empowerment was not embedded in nurses' health promotion activities ( Irvine, 2007 ).
The third common defining concept of health promotion orientation was social and health policy ( Benson and Latter, 1998 ; Whitehead, 2004 , 2006a , b , 2009 , 2011 ). These studies suggested that nurses' health promotion activities should be based on the recommendations in, for example, the World Health Organization's (WHO) charters and declarations and directives and guidance from professional and governmental organizations. However, the studies examined found that nurses were not familiar with social and health policy documents and that they did not apply them to their nursing practice ( Benson and Latter, 1998 ; Whitehead, 2011 ).
The last defining concept of health promotion orientation was community orientation ( Sheilds and Lindsey, 1998 ; Whitehead, 2004 ; Witt and Puntel de Almeida, 2008 ). These papers revealed that nurses had knowledge of community-orientated health promotion: they were expected to use health surveillance strategies, work collaboratively with other professionals and groups and respect and interact with different cultures. In addition a health promotion orientation appeared to result in nurses working more closely with members of communities, for example, being involved in voluntary work and implementation of protective and preventive health measures.
Public health orientation
Public health-orientated chronic disease prevention and treatment has traditionally been the theoretical basis of nurses' health promotion activities ( Burge and Fair, 2003 ; Berg et al ., 2005 ; Whitehead, 2006c ; Folke et al ., 2007 ; Casey, 2007b ; Irvine, 2007 ; Chambres and Thompson, 2009 ; Fagerström, 2009 ; Richard et al. , 2010 ). The first defining concept of public health orientation was disease prevention ( Berg et al ., 2005 ; Whitehead, 2006c , Folke et al ., 2007 ; Irvine, 2007 ; Fagerström, 2009 ; Richard et al. , 2010 ). According to these studies, this occurred in health promotion when the focus was on diagnosis, physical health and the relief of the physical symptoms of disease. The second defining concept of public health orientation was the authoritative approach ( Burge and Fair, 2003 ; Casey, 2007b ; Irvine, 2007 ; Chambres and Thompson, 2009 ). This approach emphasizes the need for nurses to give information to patients. In addition, the authoritative approach suggests that health promotion activities should aim to change patients' behaviour ( Irvine, 2007 ; Chambres and Thompson, 2009 ).
What type of health promotion expertise do nurses have?
The expertise of nurses with respect to health promotion was described in 16 research papers ( Robinson and Hill, 1998 ; Whitehead, 2001 , 2006b , 2007 , 2009 , 2011 ; Hopia et al ., 2004 ; Cross, 2005 ; Jerden et al ., 2006 ; Runciman et al ., 2006 ; Kelley and Abraham, 2007 ; Witt and Puntel de Almeida, 2008 ; Fagerström, 2009 ; Parker et al ., 2009 ; Goodman et al ., 2011 ; Whitehead, 2011 ). According to these papers nurses implemented a range of types of health promotion activity and applied different health promotion expertise across a wide range of nursing contexts. Depending on the context nurses are able to make use of a variety of types of expertise in health promotion. Nurses can be classified into: general health promoters, patient-focused health promoters and project management health promoters (Figure 2 ).
Concepts and examples of the types of nurses' expertise as health promoters.
General health promoters
Health promotion by nurses is associated with common universal principles of nursing. The most common health promotion intervention used by nurses is health education ( Robinson and Hill, 1998 ; Whitehead, 2001 , 2007 , 2011 ; Runciman et al ., 2006 ; Witt and Puntel de Almeida, 2008 ; Parker et al ., 2009 ). General health promoters are expected to have knowledge of health promotion, effective health promotion actions, national health and social care policies and to have the ability to apply these to their nursing practice ( Witt and Puntel de Almeida, 2008 ; Whitehead, 2009 ).
Patient-focused health promoters
There is growing recognition that different patient groups, such as the elderly or families with chronic diseases, have different health promotion needs. In promoting the health of these different groups, nurses can be regarded as patient-focused health promoters ( Hopia et al ., 2004 ; Cross, 2005 ; Jerden et al ., 2006 ; Kelley and Abraham, 2007 ; Goodman et al ., 2011 ). These studies revealed that when health promotion for patient groups who need high levels of care and treatment is required, nurses must have the ability to include health promotion activities in their daily nursing practice.
Managers of health promotion projects
Nurses should be able to plan, implement and evaluate health promotion interventions and projects ( Runciman et al ., 2006 ; Whitehead, 2006b ; Witt and Puntel de Almeida, 2008 ; Fagerström, 2009 ). Projects can facilitate the development of health promotion in nursing practice ( Runciman et al ., 2006 ). Thus, managers of health promotion projects should have advanced clinical skills and take the responsibility in supervising and leading research and development actions in nursing as well as having the ability to co-ordinate educational and developmental interventions in health-care units and communities ( Witt and Puntel de Almeida, 2008 ; Fagerström, 2009 ).
What type of professional knowledge and skills do nurses undertaking health promotion exhibit?
Nurses' knowledge of health promotion and their relevant practical skills were described in 18 research papers ( McDonald, 1998 ; Nacion et al. , 2000 ; Burge and Fair, 2003 ; Whitehead, 2003 ; Hopia et al ., 2004 ; Reeve et al ., 2004 ; Spear, 2004 ; Cross, 2005 ; Irvine, 2005 , 2007 ; Rush et al ., 2005 ; Jerden et al ., 2006 ; Casey, 2007b ; Kelley and Abraham, 2007 ; Piper, 2008 ; Witt and Puntel de Almeida, 2008 ; Wilhelmsson and Lindberg, 2009 ; Goodman et al ., 2011 ). These studies suggested that nurses' health promotion activities consisted of a variety of competencies. We classified these into multidisciplinary knowledge, skill-related competence, competence with respect to attitudes and personal characteristics (Figure 3 ).
Concepts and examples of nurses' health promotion competencies.
Multidisciplinary knowledge
Nurses' health promotion activities were often based on a broad and multidisciplinary knowledge ( Nacion et al ., 2000 ; Burge and Fair, 2003 ; Spear, 2004 ; Irvine, 2005 ; Casey, 2007b ; Witt and Puntel de Almeida, 2008 ; Whitehead, 2009 ). This included a knowledge of: health in different age groups; epidemiology and disease processes and health promotion theories. In addition, nurses need to have the ability to apply this knowledge to their health promotion activities ( Burge and Fair, 2003 ; Spear, 2004 ; Irvine, 2005 ; Runciman et al ., 2006 ; Piper, 2008 ; Witt and Puntel de Almeida, 2008 ). Nurses were also expected to be aware of economic, social and cultural issues, social and health policies and their influence on lifestyle and health behaviour ( Burge and Fair, 2003 ; Irvine, 2005 ).
Skill-related competence
Nurses must possess a variety of health promotion skills; of these, communication skills were considered to be the most important ( McDonald, 1998 ; Nacion et al. , 2000 ; Burge and Fair, 2003 ; Hopia et al ., 2004 ; Irvine, 2005 ; Jerden et al ., 2006 ; Casey, 2007b ). Nurses play a particularly important role when they encourage patients and their families to participate in decision-making related to treatment or to discuss and express their feelings about situations associated with serious illness ( Hopia et al ., 2004 ). Skill-related competence also includes the ability to support behavioural changes in patients and the skill to respond to patients' attitudes and beliefs ( Burge and Fair, 2003 ). In addition, skill-related competence involves teamwork, time management, information gathering and interpretation and the ability to search for information from different data sources ( Irvine, 2005 ; Jerden et al ., 2006 ).
Competence with respect to attitudes
Competence with respect to attitudes emerged as a positive feature of health promotion ( Whitehead, 2003 ; Reeve et al ., 2004 ; Spear, 2004 ; Cross, 2005 ; Irvine, 2005 , 2007 ; Kelley and Abraham, 2007 ; Piper, 2008 ; Wilhelmsson and Lindberg, 2009 ). Effective health promotion practice requires nurses to adopt a proactive stance and act as an advocate. An affirmative and egalitarian attitude towards patients and their families, as well as the desire to promote their health and well-being, are important attitudes with respect to health promotion activities ( Irvine, 2005 , 2007 ; Wilhelmsson and Lindberg, 2009 ). In addition, nurses who have personal experience, for example, of having had a baby, have a more positive attitude towards promoting the health of patients in the same situation ( Spear, 2004 ).
Personal characteristics
Traditionally, nurses were perceived to be healthy role models, engaging in healthy activities, not smoking and maintaining an ideal weight Burge and Fair, (2003) ; Reeve et al. , 2004 ; Rush et al ., 2005 ). In addition, personal confidence and flexibility are personal characteristics that nurses working in health promotion are expected to possess ( Burge and Fair, 2003 ; Rush et al ., 2005 ).
What factors contribute to nurses' ability to carry out health promotion?
Thirteen research papers identified features which contributed to nurses' health promotion activities ( Robinson and Hill, 1998 ; Reeve et al ., 2004 ; Jerden et al. , 2006 ; Runciman et al ., 2006 ; Whitehead, 2006b , 2009 , 2011 ; Casey, 2007a , b ; Kelley and Abraham, 2007 ; Wilhelmsson and Lindberg, 2009 ; Beaudet et al ., 2011 ; Goodman et al ., 2011 ). All of the features related to cultural aspects of the organization in which nurses work. We considered that these could be classified as either supportive or discouraging (Figure 4 ).
Concepts and examples of organizational culture associated with health promotion activities.
First, organizational culture consisted of three supportive aspects: hospital managers, culture of health and education. The hospital managers were responsible for whether health promotion was a strategically planned and whether it was considered to be of great importance ( Whitehead, 2006b , 2009 ). In addition, the hospital managers were key individuals in ensuring that health promotion activities did not conflict with other work priorities ( Jerden et al ., 2006 ; Casey, 2007a ; Beaudet et al ., 2011 ). Hospital managers also have an important role in cultivating a culture of health in the work community, for instance by prohibiting smoking during working time ( Casey, 2007a ). Education enhanced nurses' health promotion skills and health promotion projects were catalysts for health promotion in nursing practice ( Goodman et al ., 2011 ). Organizational culture included three discouraging factors. The major one was a lack of resources, including a lack of time, equipment (e.g. computers) and health education material ( Robinson and Hill, 1998 ; Reeve et al ., 2004 ; Runciman et al ., 2006 ; Casey, 2007b ; Kelley and Abraham, 2007 ; Wilhelmsson and Lindberg, 2009 ; Beaudet et al ., 2011 ). In addition, nurses may lack skills to implement health promotion in their working place ( Goodman et al ., 2011 ). Recent studies have also revealed that health promotion activities are still unclear to nurses ( Beaudet et al ., 2011 ; Whitehead, 2011 ).
Several authors have identified a need to clarify the concept of health promotion in nursing ( Goodman et al ., 2011 ; Whitehead, 2011 ). We found the concept map method useful to enhance conceptual understanding of this complex nursing phenomenon. This integrative review was intended to identify the findings of nursing-specific studies of health promotion activities published in the period 1998–2011. We identified 40 relevant English research papers. Most of these studies were published between 2005 and 2009. Combining qualitative and quantitative studies is complex and can introduce bias and error ( Whittemore and Knafl, 2005 ). The data examined herein originated from methodologically diverse research. Therefore, we should be cautious of generalizing our findings. Most of the studies were qualitative, but a broad range of health promotion activities undertaken by nurses was described. The concept map method was used to analyse the data; the results of this review are reported both as text and concept maps. Concept maps are rarely used as a data analysis tool and therefore we employed researcher triangulation (V.K., K.T. and H.T.) during the research process; this enhanced our understanding and increased scientific rigour ( Jones and Bugge, 2006 ).
We found that health promotion and public health orientation have guided nurses' health promotion activities (e.g. McDonald, 1998 ; Whitehead, 2009 ; Richard et al ., 2010 ; Povlsen and Borup, 2011 ). It was surprising that, even though there has been much public debate and research has emphasized that health policies should guide nurses' health promotion activities worldwide, health policies have little impact on nursing practice (e.g. Benson and Latter, 1998 ; Irvine, 2007 ; Whitehead, 2011 ). Nurses have a variety of types of expertise, some working as general health promoters, some as patient-focused health promoters and some as managers of health promotion projects (e.g. Whitehead, 2008 ; Witt and Puntel de Almeida, 2008 ; Fagerström, 2009 ; Goodman et al ., 2011 ). The management of health promotion projects is particularly important, although only three studies ( Whitehead, 2006b ; Witt and Puntel de Almeida, 2008 ; Fagerström, 2009 ) described the type of expertise possessed by such managers. We found that there has been great interest in nurses' health promotion competencies (e.g. Irvine, 2005 , 2007 ; Witt and Puntel de Almeida, 2008 ; Wilhelmsson and Lindberg, 2009 ). A number of studies found that nurses' health promotion activities were based on multidisciplinary knowledge (e.g. Burge and Fair, 2003 ; Irvine, 2005 ; Whitehead, 2009 ). Interestingly, knowing about the trends that will influence the population's health in the future, such as multiculturalism, new technologies and ecological changes, were not identified as nurses' health promotion competencies. Unexpectedly for us the competencies associated with attitudes were not emphasized as one of the most important competencies even though nurses should be advocates of good health. We also found that nurses' individual health-related beliefs and lifestyles are important personal characteristics in health promotion and that nurses are expected to be healthy role models (e.g. Burge and Fair, 2003 ; Reeve et al. , 2004 ; Rush et al. , 2005 ). Nurses are aware of the importance of health promotion, but organizational culture with respect to health promotion can either support or discourage them from implementing it (e.g. Reeve et al ., 2004 ; Casey, 2007a , b ; Goodman et al ., 2011 ; Whitehead, 2011 ). Managers in health-care organizations should appreciate the value of health promotion activities and ensure adequate resources for their implementation (e.g. Casey, 2007b ; Beaudet et al ., 2011 ).
According to much of the health promotion research, it appears that nurses have not yet demonstrated a clear and obvious political role in implementing health promotion activities. Instead, nurses can be considered general health promoters, with their health promotion activities based on sound knowledge and giving information to patients. Nursing is an appropriate profession in which to implement health promotion, but several barriers associated with organizational culture have a marked effect on delivery. Therefore, more research is needed to determine how to support nurses in implementing health promotion in their roles in a variety of health-care services.
V.K. was responsible for the computer-based data searches and the data analysis via the concept map method. K.T. and H.T. verified that the data searches were made properly. K.T. and H.T. verified that the concept mapping process proceeded properly and made critical appraisals in every phase of the research process. V.K. was responsible for the drafting of the manuscript. K.T. and H.T. made critical revisions to the paper for important intellectual contents, conceptualization, support in theorizing the findings and provided material support. K.T. and H.T. supervised the study.
This research received a specific grant from The Finnish Foundation for Nurse Education and The Finnish Nurses Association.
Virpi Kemppainen would like to acknowledge the support from the University of Eastern Finland, Department of Nursing Science.
Google Scholar
Google Preview
Supplementary data
Email alerts, citing articles via.
- Recommend to Your Librarian
- Journals Career Network
Affiliations
- Online ISSN 1460-2245
- Print ISSN 0957-4824
- Copyright © 2024 Oxford University Press
- About Oxford Academic
- Publish journals with us
- University press partners
- What we publish
- New features
- Open access
- Institutional account management
- Rights and permissions
- Get help with access
- Accessibility
- Advertising
- Media enquiries
- Oxford University Press
- Oxford Languages
- University of Oxford
Oxford University Press is a department of the University of Oxford. It furthers the University's objective of excellence in research, scholarship, and education by publishing worldwide
- Copyright © 2024 Oxford University Press
- Cookie settings
- Cookie policy
- Privacy policy
- Legal notice
This Feature Is Available To Subscribers Only
Sign In or Create an Account
This PDF is available to Subscribers Only
For full access to this pdf, sign in to an existing account, or purchase an annual subscription.

An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
Preview improvements coming to the PMC website in October 2024. Learn More or Try it out now .
- Advanced Search
- Journal List
- J Prev Med Hyg
- v.63(1); 2022 Mar
An assessment of nurses’ participation in Health Promotion: a knowledge, perception, and practice perspective
Herbert melariri.
1 Eastern Cape Department of Health, Port Elizabeth Provincial Hospital, Port Elizabeth, South Africa
2 School of Life and Health Sciences, University of Roehampton, London
TOLU ANDREA OSOBA
Margaret (maggie) williams.
3 Centre for Community Technology, School of Information Technology, Faculty of Engineering, Nelson Mandela University, Port Elizabeth, South Africa
PAULA MELARIRI
4 Department of Environmental Health, Nelson Mandela University, Summerstrand, Port Elizabeth, South Africa
Health promotion (HP) at the population level serves to improve health inequalities, enhance the quality of life, and ensures the provision of healthcare and related services. Nurses at all levels are charged with the task of ensuring that patients receive HP services. However, their competence in addressing this challenge needs further exploration. This study assessed the influence of HP knowledge and perceptions in nurses’ HP practice.
The study was conducted using a self-administered questionnaire among 184 nurses randomly sampled from a tertiary hospital. Questions bordered on respondents’ demographics, knowledge, perception, and practice of HP. Responses were retrieved and analysed using IBM SPSS Statistics, Version 26.0. Armonk, NY: IBM Corp, 2019.
Analysis showed a statistically significant relationship between participants demographics and possessing adequate knowledge to provide HP services. Statistically significant relationships were found amongst the following variables: ‘A holistic knowledge of disease pathology and processes are vital for effective care of patients’ and ‘education of patients on medication’ p = 0.001, ‘awareness of importance of educating patients about their condition’ and ‘patients encouraged to engage in healthy lifestyle’ p < 0.001.
Data showed that nurses’ knowledge regarding HP had a strong influence on their perception of HP. Their perception of HP in turn strongly influenced their practice of the same. Therefore, rigorous efforts must be made by governmental agencies, and organizations involved in healthcare worker training and nursing accreditation, to ensure the HP curriculum is well incorporated in nursing undergraduate training and sustained in service.
Introduction
Health Promotion involves a variety of approaches aimed at preserving the wellbeing and quality of life of people by addressing the fundamental causes of certain diseases as opposed to purely focusing on biomedical care [ 1 ]. Previously, health was seen as the very opposite of illness and diseases. With the Ottawa charter for HP in 1986, the World Health Organization effected a major change to the global view of health, not as a goal but a means to a full life [ 2 ]. As a result, HP emerged as a prime and essential activity for contemporary society with diverse initiatives and interventions designed by the World Health Organization aimed at translating the numerous concepts of HP towards practical reality [ 3 ]. Amongst the initiatives are the health-promoting hospitals (HPH) [ 4 ], health-promoting schools [ 5 ], health promotion in the sustainable development goals (SDGs) [ 6 ] and workplace-related HP [ 7 ]. These programmes have thrived due to the beneficial health outcomes emanating from them.
Today more than ever, nurses play a crucial role in HP. In addition to routine consultations and clinical duties, nurses are also involved in check-up care, patients education as well as disease prevention (DP) services [ 8 ]. In addition, nurses meaningfully contribute to several beneficial health outcomes such as educating patients on how prescribed medication works, therapeutic compliance [ 9 ], quality of life [ 8 ], and overall patient support and empowerment. To further uncover the importance of the nursing role in health promotion, Whitehead explored the current position of nursing concerning its practice, associated concept, and policy [ 10 ]. The questions raised included how much nurses know about HP and their views towards the subject of HP. Literature confirms that nurses utilize a range of expertise in delivering HP which may be generalized, patient-centered, or project management-related HP [ 8 ].
Despite the vital role nurses play in promoting population health, the prevalence of several preventable diseases continue to pose a major public health concern. In 2017, about 60% of patients presenting at all hospital emergency departments in the United States presented with preventable chronic conditions amounting to $8.3 billion in costs [ 11 ]. Relating to hospitalization, patients with chronic preventable diseases feature more frequently and stayed longer in hospital [ 12 ]. Similarly, in 2017 in India, more than 9.5 million deaths and nearly half a billion disability-adjusted life-years (DALY) were recorded [ 13 ]. Of the recorded deaths, more than 33% were considered to be preventable [ 13 ]. Within the low- and middle-income countries (LMIC), the adverse impact of the global burden of non-communicable disease (NCD) remains dire [ 14 ]. Despite widespread access to information regarding adjustable lifestyle behaviours, such knowledge does not necessarily translate to lifestyle changes [ 15 ].
South Africa is faced with a quadruple burden of disease comprising a mélange of four colliding epidemics [ 16 ]. These include communicable diseases such as HIV/AIDS and TB; maternal and child mortality; NCDs such as hypertension and cardiovascular diseases, diabetes, cancer, mental illnesses, and chronic lung diseases like asthma (mainly related to preventable lifestyle behaviour); as well as trauma and injury [ 16 ]. The quadruple burden of disease has led to the country’s adoption, in February 2013, of the 17-year visionary health plan for 2030 referred to as the national development plan (NDP) [ 16 ].
Nurses working at the various levels of healthcare delivery have a significant responsibility in HP, DP, and wellness. Due to the nursing profession’s ability to navigate the entire healthcare system worldwide, plus their role as patients’ advocates, nurses are in a position to achieve the comprehensive goal of universal health coverage (UHC) through HP. However, some reports have questioned nurses effectiveness in the discipline and practice of HP. In this study, we assessed the health promotion knowledge, perceptions, and practice of nurses in a South African tertiary hospital.
DESIGN, SAMPLE, AND RESPONDENTS
A descriptive cross-sectional design was used for this study. The population comprised of registered nurses working in a tertiary hospital in the Eastern Cape province of South Africa. The respondents were randomly selected from the overall population. Student nurses, and nurses on exchange training programs from different countries and auxiliary nurses were excluded from the study.
DATA COLLECTION
Data were collected using a self-administered structured questionnaire. Retrieved information was anonymised and only the principal researcher had access to the data. The questionnaire was adapted from a previous study [ 17 ] which had similar objectives. The questionnaire was administered over a three-month time frame between February and April 2017. Using a 95% confidence interval and a 5% error margin, a sample size of 184 was calculated. Data collection was stopped when the target sample size was achieved. Data collection was carried out by the principal investigator and a trained fieldworker.
SURVEY INSTRUMENT
The questionnaire (supplementary file 1) comprised of 22 closed-ended questions divided into four sections. Section A comprised of seven questions focused on demographics including sex, age group, registration status as a nurse, and duration of registration as a nurse. Section B (questions 8-9) elicited information on knowledge; Section C (questions 10-15) concentrated on nurses’ perceptions towards health promotion, while section D (questions 16-22) centered on nurses’ practice of health promotion.
DATA ANALYSIS
Data was analyzed using IBM SPSS Statistics for Windows, Version 26.0. Armonk, NY: IBM Corp, 2019. Simple descriptive analysis was conducted on all four sections (demographics, knowledge, perception, and practice) for which data were retrieved. Bivariate analysis was conducted to establish the relationship between demographics and knowledge, perception, and practice. A similar analysis was conducted to assess the relationship between perception and practice, knowledge, and practice, as well as knowledge and perceptions.
The study protocol received ethics approval from both the University of Roehampton, London, and the Research Ethics Committee (Human) (REC-H) of the Nelson Mandela University (NMU), Ref: H16-HEA-NUR-EXT-003. Every respondent signed an informed, written consent form prior to participation. The study comprised of a survey of non-vulnerable adults, and there was no potential for coercion of respondents, distress, loss of work time, or damage to professional reputation.
BASELINE CHARACTERISTICS
A total of 184 nurses responded to the questionnaire. Female nurses comprised 82.6% (n = 152), while males comprised 7.6% (n = 14) of the respondents. Genders for 9.8% (n = 18) were not specified. Most nurses, 72% (n = 133) were 40 years or above. Of the respondents, 35.9% (n = 66) have been registered for 10 years or less as nurses. Analysis on each variable is relative to the total responses Received: that variable. A descriptive summary of the variables has been presented in Tables I-IV .
Knowledge, perception and practice of health promotion.
Relationship between responses on health promotion perception and practices by nurses
SA: Strongly Agree; A: Agree; N: Neutral; DA: Disagree; SDA: Strongly disagree.
Relationship between Knowledge and Practice
Relationship between nurses’ knowledge and Perception regarding HP
KNOWLEDGE, PERCEPTION AND PRACTICE OF HEALTH PROMOTION
Of the participating 184 nurses, 56.0% (n = 103) agreed to having adequate knowledge regarding the conditions patients present within their units and their ability to provide health promotion services. A total of 63.6% (n = 117) respondents strongly held the perception that health education and counselling from nurses could enhance patients’ health, while 51.6% (n = 95) encourage their patients to observe fitness assessments and health screening. A descriptive summary of the respondents has been presented ( Tab. I ).
BIVARIATE ANALYSIS OF RELATIONSHIPS AMONG OUTCOMES
Results show that at a 5% significance level, there is a significant association between the professional registration duration of a nurse and them having adequate knowledge to provide HP services regarding the conditions patients present with in their unit (p = 0.015). Similarly, the demographic variable ‘age range’ has a statistically significant relationship with the perception that the hospital is an ideal place for HP to occur (p = 0.006). No statistical association was identified between nurses’ demography and practice.
In a comparative assessment of nurses’ perceptions and their HP practices as outcome variables, 21 variables were statistically significant ( Tab. II ). Of the 21 emerging factors, four emerged between the perception that a holistic knowledge of disease processes is a pre-requisite for patient care when compared with HP practice; four from the perception that a hospital is an ideal place for HP when compared with practices; four factors were observed from the perception that patients who engage in an unhealthy lifestyle will not benefit from HP when compared with HP practice; two from the perception that health education and counselling from nurses could enhance patients’ health when compared with HP practice; and seven factors from the perception that patients do not want health education from nurses when compared with HP practice. No statistically significant factor emerged from the perception that health promotion is a waste of time when compared with HP practice.
Comparison of the relationship between Knowledge and Practice yielded 11 statistically significant relationships ( Tab. III ). A breakdown of the 11 factors shows that nurses having adequate knowledge necessary for HP provision and practice had six significant factors, while the relationship between nurses being aware of the importance of providing health education (HE) to patients with HP practice produced five statistically significant relationships. The results showed that there were significant associations between ‘having adequate knowledge regarding the conditions patients present with in this unit to provide HP services’ and educating patients about their disease condition’, p < 0.001; ‘awareness of the importance of educating patients about their condition’and ‘patients encouraged to engage in healthy lifestyle’ p < 0.001.
Table IV shows the relationship between nurses’ knowledge and perception towards HP. The analysis showed nine significant associations emerging including: ‘having adequate knowledge regarding the conditions patients present with in this unit to provide HP services’ and ‘HE, advise and counseling from nurses could positively enhance patients health’, p < 0.001; ‘awareness of the important of educating patients about their condition’ and ‘patients do not want HE from nurses’, p < 0.001.
This study provides an assessment of nurses’ views regarding their knowledge, perception, and practice towards health promotion in a South African tertiary hospital. The data analysis revealed that nurses agreed to having adequate knowledge regarding their patients’ disease condition to provide adequate health promotion; that hospital is an ideal place to provide health promotion; and that they do encourage their patients to engage in the healthiest lifestyle they can attain. They therefore deserve a strong support system to enable them to sustain and improve their role in HP.
Findings from this study show that the duration of registration as a nurse was associated with adequate knowledge, indicating that experience adds to the nurses know-how and expertise [ 18 ]. Lartey et al. reported on the wealth of knowledge and wisdom associated with experienced nurses as being critical in the provision of high quality care to patients and their family [ 19 ]. Though this benefit of experience and adequate knowledge resulting from experience could be generalized in some cases, it is mostly discipline-specific. For example, it has been observed that nurses without exposure to health promotion and health literacy, regardless of their nursing experience, lack requisite knowledge in these disciplines [ 20 ].
The present study revealed the influence of nurses HP perception on their practice of HP. For example, the nurses who had the perception that holistic knowledge of disease pathology and processes are vital for effective care of patients were more inclined to educate their patients about adherence to medication, the importance of check-ups, and engagement in a healthy lifestyle. In a similar study by Al-Noumani et al., (2019), the authors demonstrated that adherence to medication was greater among those that believed in the importance of medication [ 21 ]. In the study of Ojong, Nsemo and Aji, (2020) conducted in Nigeria, it was observed that despite good knowledge and perception towards routine check-ups, there was still a poor practice of check-up care [ 22 ], which is an essential component of HP. The finding of good check-up practice in the current study may be related to the study context, in our case, a public tertiary hospital in South Africa where the public healthcare is solely funded by the state [ 23 , 24 ], and free transport services to and from hospitals are provided to indigent patients living in the rural areas [ 25 ]. A major fact regarding perception is its ability to become reality and guide people’s behavior [ 26 ]. In this study, the perception of the respondents is that holistic knowledge of disease pathology is a prerequisite for HP provision. This perception was formed based on their formal training and lived experience from practice. Furthermore, this study identified the perception “hospital is an ideal place for HP” as being associated with nurses using their smart devices to access supportive information during practice in order to educate patients about medication and the importance of regular check-ups. Evidence abounds regarding the efficacy of the HP effectiveness of nurses linked to organizational culture [ 8 ] as demonstrated in hospital settings [ 15 ]. Educating patients within healthcare institutions is a fundamental aspect of healthcare delivery. The educational roles of nurses therefore serve as a determinant in shared decision-making between nurses and patients regarding treatment adherence, improving the patients degree of satisfaction with service provision, and enhanced care.
Credible sources have been noted to be key players in the dissemination of public health messages amongst various groups [ 27 ]. Nurses occupy such a position among patients and are well suited to provide HP. Our results corroborate with the findings of Timmers et al., (2020) which demonstrated that educating patients at the point of care using prompt medical information accessed via smartphones and similar devices does enhance treatment compliance, satisfaction, and improves the eventual health outcome [ 28 ]. Although our study did not show a significant relationship between ‘hospital is an ideal place for HP’ and ‘educating patients about their disease condition’, the study of Nikitara et al., (2019) did indicate that nurses who are actively involved in educating patients with diabetes mellitus empower the patients to optimise management of their disease condition [ 29 ]. The reason for our finding of non association between hospital is an ideal place for HP and education of patient concerning their health condition could be related to the nurses lack of knowledge about specific disease entities [ 29 ].
The influence of knowledge among nurses correlated positively with regards to their HP practice in this study. It was noted that there was a statistically significant relationship between the provision of necessary guidance regarding diet and lifestyle to patients and adequate knowledge regarding the medical condition of the patients. Sufficient knowledge [ 30 , 31 ] is required in order for nurses to guide patients about smoking cessation, diet, and physical activity. However, in some hospital settings, nurses argue that it is the responsibility of specialists, such as dieticians, to provide dietary counselling to patients [ 30 ]. Despite this contention, enhancing the knowledge of nurses has proven to be a cost-effective strategy towards addressing the ever-increasing cost of healthcare [ 32 ]. In addition, optimum training and knowledge empowerment can embolden nurses to fully discharge their HP roles [ 32 ], including adequately guiding their patients on matters relating to necessary and health inducing diet and lifestyle changes.
This study was aimed at assessing the influence of HP knowledge and perceptions in the practice of HP amongst nurses working in a tertiary hospital. The data revealed that nurses’ HP knowledge played a key role in influencing their perception of, and eventual, HP practices. Health promotion is an important public health discipline necessary, and essential, for the achievement of universal health coverage. Nurses, due to their expertise and being regularly in touch with patients, especially those with chronic non-communicable diseases, occupy a distincitve place both in leadership and provision of HP services to their patients. A rigorous educational programme is required, in both undergraduate training and in the form of in-service training, to ensure that their knowledge of HP is updated. Future research is encouraged to interrogate the possibility of nurses achieving and sustaining a model that can bring about a realistic reform in HP.
Acknowledgements
The authors would like to acknowledge the Eastern Cape Department of Health, South Africa for granting access and space for this study, and the registered nurses that participated. No funding was received for this study from any funding agency.
Figures and tables
Conflict of interest statement
The authors declare no conflict of interest.
Authors’ contributions
Conceptualization: HM; Methodology: HM, TAO, MW, PM; Software: HM, PM; Validation: HM, TAO, MW, PM; Formal analysis: PM, HM; Investigation: HM; Data Curation: HM, PM; Writing - Original Draft: HM; Writing - Review & Editing: HM, TAO, MW, PM; Visualization: HM, TAO, MW, PM; Supervision: TAO, MW.
Want to create or adapt books like this? Learn more about how Pressbooks supports open publishing practices.
Week 13: Health Promotion and Roles of the Nurse
Unit Learning Objectives
At the end of this chapter, the learner will:
1. Define the scope of health promotion and disease prevention. 2. Discuss the nurse’s role in promoting health and preventing illness. 3. Recognize the importance of patient education on health promotion and disease prevention. 4. Discuss elements of effective patient teaching and learning. 5. Demonstrate effective planning and delivery of patient education
Overview of the Chapter
This chapter will include what is health promotion and prevention. Health promotion and disease prevention is very important and as as nurses, it is one of the role that the nurses implement everyday. It is important to provide patient education for health promotion and disease prevention. This chapter includes tools to provide patient education and provide effective patient teaching. This chapter will include concepts of health promotion, disease prevention, nurse’s role in teaching patients on health promotion.
Introduction
What do we understand by the terms health and health promotion?
Health: When broadly defined, it is a state of complete physical, mental and social wellbeing not merely the absence of disease or infirmity. According to this definition physical, social and psychological factors all contribute to health.
Health promotion: According to the Ottawa Charter, health promotion is defined as the process of enabling people to increase control over, and to improve, their health. Health promotion is aimed at reducing the underlying causes of ill-health so that there is a long term reduction in many diseases.
The 1984 WHO revised definition of health defined it as “the extent to which an individual or group is able to realize aspirations and satisfy needs, and to change or cope with the environment. Health is a resource for everyday life, not the objective of living; it is a positive concept, emphasizing social and personal resources, as well as physical capacities. Thus, health referred to the ability to maintain homeostasis and recover from insults. Mental, intellectual, emotional, and social health referred to a person’s ability to handle stress, to acquire skills, to maintain relationships, all of which form resources for resiliency and independent living.
Exercises : Self-assessment
Write down your responses to the following questions:
- What does health mean to you?
- How important is health to you?
- What do you do (if anything) to stay healthy?
I. Health Promotion
Health promotion and disease prevention through population-based interventions, including action to address social determinants and health inequity from the World Health Organization (2023).
A. Disease prevention
Primary prevention are those preventive measures that prevent the onset of illness or injury before the disease process begins. Services and activities include:
- Vaccination and post-exposure prophylaxis of children, adults and the elderly;
- Provision of information on behavioral and medical health risks, and measures to reduce risks at the individual and population levels;
- Inclusion of disease prevention programmes at primary and specialized health care levels, such as access to preventive services (ex. counselling)
- Nutritional and food supplementation
- Dental hygiene education and oral health services.
- Education about healthy and safe habits (e.g. eating well, exercising regularly, not smoking)
Secondary prevention are those preventive measures that lead to early diagnosis and prompt treatment of a disease, illness or injury to prevent more severe problems developing. Here health educators such as Health Extension Practitioners can help individuals acquire the skills of detecting diseases in their early stages. This includes activities such as:
- Population-based screening programmes for early detection of diseases; screening for high blood pressure and breast self-examination.
- Provision of maternal and child health programmes, including screening and prevention of congenital malformations; and
- Suitably modified work so injured or ill workers can return safely to their jobs.
Tertiary prevention are those preventive measures aimed at rehabilitation following significant illness. At this level health services workers can work to retrain, re-educate and rehabilitate people who have already developed an impairment or disability.
- Cardiac or stroke rehabilitation programs, chronic disease management programs (e.g. for diabetes, arthritis, depression, etc.)
- Support groups that allow members to share strategies for living well
- Vocational rehabilitation programs to retrain workers for new jobs when they have recovered as much as possible.
Exercises: Read the list of the three levels of prevention again. Think about your experience of health education, whether as an educator or recipient of health education.
- How do you think health education can help with the prevention of disease?
- Do you think it will operate at all these levels?
- Think of an example of possible health education interventions at each level where health education can be applied.
B. Levels of Care: Differences Between Primary, Secondary, Tertiary, and Quaternary Care
In medicine, levels of care refer to the complexity of the medical cases doctors treat and the skills and specialties of the providers. Levels are divided into four categories.
Primary care is when you consult with your primary care provider. Secondary care is when you see a specialist such as an oncologist or endocrinologist. Tertiary care refers to specialized care in a hospital setting such as dialysis or heart surgery. Quaternary care is an advanced level of specialized care.
:max_bytes(150000):strip_icc():format(webp)/VWH-MichelaButtignol-DifferencesBetweenPrimarySecondaryTertiaryCare-Standard-81aff211ec5c444b9de025c48d9bd416.jpg "role of nurse in health promotion essay")
Levels of care refer to the complexity of medical cases, the types of conditions a physician treats, and their specialties.
- Primary care involves your primary healthcare provider. You see them for things like acute illnesses, injuries, screenings, or to coordinate care among specialists.
- Secondary care is the care of a specialist. These specialists may include oncologists, cardiologists, and endocrinologists.
- Tertiary care is a higher level of specialized care within a hospital. Similarly, quaternary care is an extension of tertiary care, but it is more specialized and unusual.
II. The Role of the Nurse
Registered nurses have the unique ability to work in a variety of environments and specializations. From bedside care to administrative work to home care and travel nursing, RNs aren’t limited to traditional hospital roles. Find out more about the career opportunities available to you as an RN. Review the different roles and opportunities nurses available. You may click on the different careers such as inpatient, outpatient or alternate to understand your roles and responsibilities in each setting or role. https://www.registerednursing.org/nursing-careers/#inpatient
A. Health Education can be applied at all three levels of disease prevention and can be of great help in maximizing the gains from preventive behavior .
- For example at the primary prevention level — you could educate people to practice some of the preventive behaviors, such as having a balanced diet so that they can protect themselves from developing diseases in the future.
- At the secondary level, you could educate people to visit their local health center when they experience symptoms of illness, such as fever, so they can get early treatment for their health problems.
- At the tertiary level, you could educate people to take their medication appropriately and find ways of working towards rehabilitation from significant illness or disability.
B. Health promotion
- Policies and interventions to address tobacco, alcohol, physical activity and diet (e.g., FCTC , DPAS , alcohol strategy and NCD best-buys)
- Intersectoral policies and health services interventions to address mental health and substance abuse
- Strategies to promote sexual and reproductive health, including through health education and increased access to sexual and reproductive health, and family planning services
- Strategies to tackle domestic violence, including public awareness campaigns; treatment and protection of victims; and linkage with law enforcement and social services.
C. Support mechanisms for health promotion and disease prevention
- Multisectoral partnerships for health promotion and disease prevention
- Educational and social communication activities aimed at promoting healthy conditions, lifestyles, behavior and environments (see EPHO VII)
- Reorientation of health services to develop care models that encourage disease prevention and health promotion
- Risk communication.
https://www.emro.who.int/about-who/public-health-functions/health-promotion-disease-prevention.html
III. Patient Education
Patient education is defined as “any set of planned educational activities , using a combination of methods (teaching, counseling, and behavior modification), that is designed to improve patient’s knowledge and health behaviors”(Friedman, Cosby, Boyco, Hatton-Bauer,&Turnbull, 2011). Nurses must have a basic understanding of the principles and process of teaching and learning to carry out their professional practice responsibilities effectively. All nursing practices acts including teaching within the scope of nurse’s responsibilities to assist patients to maintain optimum level of wellness and manage illness.
The purpose of patient education is to increase patient’s competence and confidence for self-management. Effective patient education can result increase patient satisfaction, improved quality of life, ensure continuity of care and decreased anxiety. Other benefits are reduced complications, promotion of adherence to treatment plan, maximize independence and empower planning own care.
A. Patient education Process : is a systematic, sequential, logical, scientifically based, planned course of action consists of learning and teaching. This education process is compared to nursing process. It depicts the steps of the nursing process parallel to the education process.
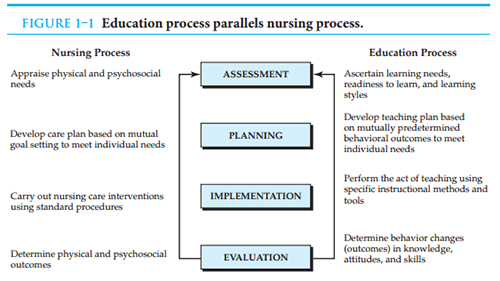
Adapted from “essentials of patient education” S.B. Bastable
B. Nursing Process
The patient education process has 4 equal components to be addressed by the nurse: assessment, planning, implement, and evaluation. Excellent patient education is an “art” and “science” using nuances and evidence-based strategies to effectively educate. The assessment and evaluation components often use nuanced approaches (motivational interviewing, teach back) to engage the patient/caregiver respectfully, whereas planning and implementation rely more on evidence-based strategies such as the patient education assessment of materials. Nurses should provide education that is simple, patient centered, and multimodal to meet the health literacy needs of patients/caregivers.
C. Learning Domains
Teaching and instructions are deliberate interventions that involve sharing of information to meet intended learner outcomes in cognitive, affective and psychomotor domains according to an educational plan.
- Cognitive : Memorization, recall, comprehension, ability to analyze, apply ideas & evaluate ideas EXAMPLE: understanding traffic laws, ability to recall & apply learned information when driving. (Lecture)
- Affective : Responding to new ideas, demonstrating commitment to new ideas, & integrating new ideas into their value system. EXAMPLE: Driving when rested, pulling over when tired, driving sober (Discussion)
- Psychomotor: Sensory awareness of cues involved in learning as well as imitation & performance of skills & creation of new skills. EXAMPLE: Successfully driving using both feet & hands appropriately. A patient changes his dressing after observing it done by nurse the day before. (Demonstration: Successfully giving yourself an insulin injection after acquiring the skills to do so.)
The ASSURE model is developed to help nurses to organize and carry out education process.

D. Barriers to Teaching
Factors interfering with the health professional’s ability to teach include:
- Lack of time
- lack of motivation and skill
- negative influence of the environment (lack of space, and privacy, noise)
- absence of third-party reimbursement
- low priority status of client education
- lack of confidence and competence
- questionable effectiveness of client education
- documentation difficulties
- Sensory deficits include: impaired or loss of vision and hearing
- language barrier and culture Barrier
- Literacy Barrier: ability to read, write and speak in English and compute and solve problems at levels of proficiency necessary to function on the job and in society, to achieve one’s goals, and to develop one’s knowledge and potential.
- Physical and Environmental Barriers
- Learning Styles
- Teaching Methodologies
For effective delivery of health information and education, the nurse must be aware of the barriers that can impede the patient’s ability and readiness to learn. Awareness of the potential barriers of literacy, culture, language, and physiological factors will help the nurse determine what tools he or she may need to assist in the delivery of information. Awareness of one’s biases and prejudices and overcoming them will assist in the education process.
- Understand subject Matter
- Careful Assessment of patient’s Learning Needs
- Control Environment
- Use Appropriate Teaching Methods
IV. Application in Practice
Exercises: Patient education using teach-back method.
- Watch the video below
- What did you observe in this scenario that relates to the use of medical terminology when giving patient education?
- How did the nurse apply the nursing process in this video?
Exercises: Patient Teaching/Nursing Process
Instructions:
Divide into 4 groups with 2-3 students each. Each group will represent one part of the Nursing Process.
- Group A: Assessment
- Group B: Planning
- Group C: Implement
- Group D: Evaluate
- Have each group present their “step” of the Nursing Process in the teaching plan from the case study below. Each group will have 5 minutes to present their information.
- Encourage the students to ask questions to their classmates and to add any additional thoughts that their group may have identified in each part of the nursing process.
Daniel is a 16-year-old boy who was taken to the emergency room (E.R) from school by ambulance after he collapsed during a baseball game. Daniel is one of 3 pitchers on the team. His younger sister, age 10, was at the game and witnessed her brother’s injury.
In the E.R. Daniel was seen by several specialists who ran multiple tests. He was admitted to the hospital and subsequently diagnosed with Type 1 Diabetes Mellitus.
Daniel along with his parents, was told that diet alone will not regulate the disease and daily Insulin Injections must be administered.
Create a teaching plan on how to administer Insulin Injection for Daniel and his parents.
V. Reflections
Key Takeaways
Type your key takeaways here.
VI. Recommended Resources
Health Disparities: https://www.cdc.gov/healthyyouth/disparities/index.htm
Health Promotion Activities: https://www.cdc.gov/chronicdisease/programs-impact/health-promotion/index.htm
Patient-education tips for new nurses: https://journals.lww.com/nursing/Fulltext/2013/10000/Patient_education_tips_for_new_nurses.24.aspx
National Center for Health Promotion and Disease Prevention: https://www.prevention.va.gov/
Health Promotion and Disease Prevention Interventions for the Elderly: A Scoping Review from 2015–2019: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7432678/pdf/ijerph-17-05335.pdf
health.gov: healthy PEOPLE 2023 :https://health.gov/
Impact Quick Facts: https://www.cdc.gov/chronicdisease/pdf/impacts-H.pdf
What is Nursing?: https://www.nursingworld.org/practice-policy/workforce/what-is-nursing
Duties of a Registered Nurse | in a Hospital and Nursing Home: https://www.registerednursern.com/duties-of-a-registered-nurse-in-a-hospital-and-nursing-home/
Tackling the Teach-Back Method: https://engage.healthynursehealthynation.org/blogs/8/4537
References and Attributes
Gewurtz, R., Moll, S., Letts, L., Lariviere, N., Levasseur, M., & Krupa, T. (2016). What you do every day matters: A new direction for health promotion. Canadian Journal of Public Health , 106 (2), e205-e208. https://doi .org/ 10.17269/CJPH.107.5317
The World Health Organization (2023). Retrieved from https://www.emro.who.int/about-who/public-health-functions/health-promotion-disease-prevention.html
Bastable, S. B. (2016). Essentials of patient education . Jones & Bartlett Learning.
Differences Between Primary, Secondary, Tertiary, and Quaternary Care: Retrieved from https://www.verywellhealth.com/primary-secondary-tertiary-and-quaternary-care-2615354
Burke, A. (2020, January 15). Collaboration with interdisciplinary team: NCLEX-RN . RegisteredNursing.org. https://www.registerednursing.org/nclex/collaboration-interdisciplinary-team/#collaborating-healthcare-members-disciplines-providing- client -care ↵
J. Baker (n. d): 1.2: Three Levels of Health Promotion/Disease Prevention LibreTexts platform https://med.libretexts.org/Bookshelves/Health_and_Fitness/Contemporary_Health_Issues_(Baker)/01%3A_Introduction_to_Personal_Health/1.02%3A_Three_Levels_of_Health_Promotion_Disease_Prevention
The Novice Nurse's Guide to Professional Nursing Practice Copyright © by Kunjamma George and rbertiz is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License , except where otherwise noted.
Share This Book
- Cancer Nursing Practice
- Emergency Nurse
- Evidence-Based Nursing
- Learning Disability Practice
- Mental Health Practice
- Nurse Researcher
- Nursing Children and Young People
- Nursing Management
- Nursing Older People
- Nursing Standard
- Primary Health Care
- RCN Nursing Awards
- Nursing Live
- Nursing Careers and Job Fairs
- CPD webinars on-demand
- --> Advanced -->

- Clinical articles
- CPD articles
- CPD Quizzes
- Expert advice
- Clinical placements
- Study skills
- Clinical skills
- University life
- Person-centred care
- Career advice
- Revalidation
CPD
Effective approaches to health promotion in nursing practice, adele phillips senior lecturer in health promotion and public health, school of allied and public health professions, faculty of health and wellbeing, canterbury christ church university, canterbury, kent, england.
• To recognise the role of individuals’ lifestyles, the environment, healthcare organisations and biology in the prevention of illness and the maintenance of population health
• To understand how health promotion approaches can be embedded in your role and enhance the overall effectiveness of your practice
• To count towards revalidation as part of your 35 hours of CPD, or you may wish to write a reflective account (UK readers)
• To contribute towards your professional development and local registration renewal requirements (non-UK readers)
This article defines the concept of health promotion and explains why it is essential for nurses to embed health promotion aims and values in their practice. It discusses how health promotion contributes to the improvement and maintenance of population health and contemporary public health agendas in the UK and worldwide. Using several practical activities, this article aims to encourage nurses to identify their own approach to promoting health in their professional role, consider how they can implement ‘Making Every Contact Count’ with the patients they care for, and enhance the overall effectiveness of their practice.
Nursing Standard . doi: 10.7748/ns.2019.e11312
This article has been subject to external double-blind peer review and checked for plagiarism using automated software
None declared
Phillips A (2019) Effective approaches to health promotion in nursing practice. Nursing Standard. doi: 10.7748/ns.2019.e11312
Accepted 19 November 2018
Published online: 04 March 2019
behaviour change - health inequalities - health literacy - health promotion - lifestyles - patient education - patient empowerment - patients - public health - wellbeing
User not found
Want to read more?
Already have access log in, 3-month trial offer for £5.25/month.
- Unlimited access to all 10 RCNi Journals
- RCNi Learning featuring over 175 modules to easily earn CPD time
- NMC-compliant RCNi Revalidation Portfolio to stay on track with your progress
- Personalised newsletters tailored to your interests
- A customisable dashboard with over 200 topics
Alternatively, you can purchase access to this article for the next seven days. Buy now
Are you a student? Our student subscription has content especially for you. Find out more

03 April 2024 / Vol 39 issue 4
TABLE OF CONTENTS
DIGITAL EDITION
- LATEST ISSUE
- SIGN UP FOR E-ALERT
- WRITE FOR US
- PERMISSIONS
Share article: Effective approaches to health promotion in nursing practice
We use cookies on this site to enhance your user experience.
By clicking any link on this page you are giving your consent for us to set cookies.
Health Promotion in Nursing Analysis Essay
Introduction, purpose in nursing practice, roles and responsibilities, implementing health promotion, comparisons, reference list.
Health promotion has become imperative in the control and prevention of diseases. The concept of integrating health promotion in all aspects of life has been informed by the high prevalence of diseases and conditions that are preventable. The creation of a healthy lifestyle has developed tremendously in the last few decades as observed in the process of maintaining health and delivery of quality healthcare. The social and economic impacts of these conditions are enormous to the family and other countries, particularly in the developed world. In this essay, a review of the literature of three journals will be put in perspective with a view of knowing the definition of health promotion, and the roles of the nurses in the overall implementation program.
Health promotion can be defined using several definitions depending on the contextual application in nursing. In Richard et al (2008) article, health promotion is regarded as the measures put in place to ensure that individuals are cushioned against receiving injuries or various debilitating conditions. With regard to this, interventions and other preventive measures are put in place to safeguard the well-being of elderly persons. In fact, the researchers set to assess the level of utilization of primary prevention in several community settings where elderly individuals are catered for using theoretical approaches. In their article, Mao and Anastasi (2010) discuss the vital role and implications of the diagnosis and the overall management of endometriosis in women. As part of the nurses’ role, the researchers acknowledge the useful roles played by advanced nursing practice in the overall prevention and mitigation of the occurrence of terrible effects. Health promotion thereby focuses on providing adequate diagnostic measures coupled with treatment procedures aimed at curtailing the progress of a disease. In this case, the researchers devise activities that ensure there is a reduction in severity. Bouman et al (2008) look at the effects that home visiting programs would offer in terms of health-related measures to individuals suffering from terminal or debilitating conditions. The majority of these conditions are untreatable thus occasioning the need to offer palliative care coupled with emotional support. Using random controlled trials, the researchers try to understand the impact emotional and psychosocial support activities have on bettering the lives and health of terminally ill persons. According to the article, health promotion refers to those interventions directed to sick individuals with the aim of checking the occurrence of complications and deterioration of the overall health of the patients.
Nursing practice has evolved greatly in the last few decades whereby nurses have become more involved in the management of the patients. In view of the change in the preferences of patients and advancements in technology, nursing practice has transformed to accommodate cultural practices, technology, and more professionalism (Bouman et al, 2008). The intertwining of disease causation with economic and social life has occasioned the nurses to act as important avenues in providing guidance and instilling knowledge on disease causation to individuals. Health promotion has therefore become useful in breaking the disease causation cycle (Mao & Anastasi, 2010). Nurses are also bolstered thus enabling them to disseminate information on patients and utilize evidence-based practices that offer lasting impacts on diseases prevention and management. More importantly, nursing practice is enhanced since the nurses receive useful tips on the approach and information to be disseminated to the individuals and at which stage of the disease.
A paradigm shift has taken place in the nursing profession in terms of responsibilities according to the nurses. Due to their close interaction with the patients, the nurses’ responsibilities have soared to accommodate emotional and psychological support to patients. Moreover, nurses have become more involved in palliative care and offering culturally competent care. In this regard, nurses remain the major avenue that will ensure the success of health promotion due to the immense time they spend with the patients (Richard et al, 2008)
Nursing roles cut across all vital processes offered in healthcare facilities thereby bringing into fore specialization in various fields. Improvement in the curriculums and training has equipped the nurses with vital and immense knowledge that enhances their capabilities to advise and share vital information at any level and setting. Their holistic training and exposure give them an edge over other health professionals since they are equipped with communication skills and the basics of disease etiology.
Health promotion aims to lower the risks, the occurrence of disease, and lessen the complications occasioned by the diseases. All three levels of health promotion aim to lower the number of suffering patients undergo. In addition, the three levels involve actions that are overly directed in ensuring the recipients of the information are empowered through the acquisition of vital skills. The individuals are thus empowered to influence their actions towards achieving healthy living hence reorienting the healthcare services delivery.
Health promotion in nursing has therefore played a crucial role in enhancing their responsibilities and shaping the profession. In fact, health promotion has become an integral component of the nursing profession as espoused in the reviewed articles and thus the need to strategies on ways of integrating it into overall health programs.
Bouman, A., Rossum, E., Ambergen, T., Kempen,G. & Knipschild, P. (2008). Effects of a Home Visiting Program for Older People with Poor Health Status: A Randomized, Clinical Trial in the Netherlands. Journal of American Geriatric Society, 56, 397–404.
Mao, A. & Anastasi, K. (2010). Diagnosis and management of endometriosis: The role of the advanced practice nurse in primary care. Journal of the American Academy of Nurse Practitioners, 22, 109–116.
Richard, L., Gauvin, L., Gosselin, C., Ducharme, F., Sapinski, J. & Trudel, S. (2008). Integrating the ecological approach in health promotion for older adults: a survey of programs aimed at elder abuse prevention, falls prevention, and appropriate medication use. International Journal of Public Health , 53, 46–56.
- Chicago (A-D)
- Chicago (N-B)
IvyPanda. (2022, March 22). Health Promotion in Nursing Analysis. https://ivypanda.com/essays/health-promotion-in-nursing-analysis/
"Health Promotion in Nursing Analysis." IvyPanda , 22 Mar. 2022, ivypanda.com/essays/health-promotion-in-nursing-analysis/.
IvyPanda . (2022) 'Health Promotion in Nursing Analysis'. 22 March.
IvyPanda . 2022. "Health Promotion in Nursing Analysis." March 22, 2022. https://ivypanda.com/essays/health-promotion-in-nursing-analysis/.
1. IvyPanda . "Health Promotion in Nursing Analysis." March 22, 2022. https://ivypanda.com/essays/health-promotion-in-nursing-analysis/.
Bibliography
IvyPanda . "Health Promotion in Nursing Analysis." March 22, 2022. https://ivypanda.com/essays/health-promotion-in-nursing-analysis/.
- Neuropsychiatry: Hill's Criteria for Causation
- Occupational Health and Safety: Accident Causation Models
- Accident Causation Theories and Frameworks
- Causation in Epidemiology: Clinical Pharmacology
- Causation in Criminal Liability and Reforms
- The Major Theories of Crime Causation
- Sociology. The Theory of Causation by Spencer
- Basic Models of Accident Causation
- Causation and Causal and Etiologic Factors of Mental Illness Differences
- Major Theories of Crime Causation
- Health Care Proposals in the United States
- U.S. Health Care Policy on Counterfeit Drugs
- King Edgar NHS Hospital's Trust Issues
- Health Care Reform Advocacy
- National Patient Safety Goals: Overview
- +1 406 637 6982
- [email protected]
Nursing Writing Services - Blog
-nurse student companion-.

Nurses Role in Health Promotion Essay
Health promotion is a fundamental factor in the well-being of everyone. It is the "procedure of enabling people to have control of and develop their health" (WHO, 1986). It is important for individuals to take responsibility for their health by eating healthy and staying active but nurses are a vital ingredient in promoting wellness and a healthy lifestyle.Some do not know the best way to stay fit and rely on nurses for guidance. This discussion will reveal the different roles by a nurse in promoting health in various work environments.
Nurses Role in Health Promotion for Patients
Nurses' role in health promotion has a high rate of success since they work in various settings and interact with people from different cadres. They look after patients in healthcare facilities, patient homes and within the community. Most of the time, they perform a diagnosis and give the instructions to care givers hence they are the people to spend more time with the patients. Nurses therefore play a “key role in promoting patient health” (Irvine, 2005). The long hours they spend providing care enables them to understand other life aspects by patients in addition to the ailment they are recovering from to determine if their lifestyle is healthy. They are also able to follow up if a patient is following the instructions and advice on improving the quality of life.
Nurses interact widely with patients at different places getting an environment to educate and discuss the health status than the physicians who only meet with a patient in hospitals and clinics. It is the reason behind the argument that nurses have a potentially critical role in promoting patients’ health (Irvine, 2005). A good example is that it is the responsibility of nurses to provide continuity of care to a patient after a hospital discharge. Usually a community nurse will follow up on the progress of recovery. It will include educating the patients on how to live a healthier life and prevent diseases. For patients who are under the care of their families, a nurse also becomes an agent of healthy promotion to other people in the home. The ultimate point is that nurses can reach everyone.
Nurses Role in Health Promotion in Communities
To strengthen communities and to create a supportive environment are some of the pillars for supporting the initiative by world health organization (WHO) for having "health for all."
In every community, there is a nurse, but it is not usual to have doctors in the smaller neighborhoods. The proximity of nurses to members of the community enables them to be educators, advocates, and coordinators of promotion of health including lifestyle changes. (Blais& Hayes, 2011). Usually, it is upon nurses to educate their patients about the benefits of observing a healthy lifestyle including the essential habits that people neglect such as exercising, taking a balanced diet, exercising and getting an adequate amount of sleep.
Wondering where to buy Best Nursing Assignments Writing Services ? Try nursingwritingservices.com today!.
A nurse can coordinate a healthy plan with patients to substitute unhealthy choices with wholesome and beneficial alternatives. For instance, nurses are essential in creating a healthy meal plan and regimen for exercising to help obese persons in reducing their weight.
Another critical role that nurses play in promoting health is to encourage members of the community to attend regular screenings and early detection diagnostic tests (Blais& Hayes, 2011). The motivation helps in early detection of terminal illnesses such as cancer before reaching life threatening level.
Nurses Role in Health Promotion By Immunization
Immunization is a critical element and cost effective way of promoting preventive care. According to WHO, vaccination prevents up to three million deaths per year. Nurses play an essential role in advancing the health of children by administering an immunization.
"When functioning in a health promotion model" (Rankin 2005), each contact that nurse have with patients or their families is an opportunity to educate their patients or families. They advise parents on the excellent ways of taking care of their kids and coordinate childhood immunization programs in their respective areas. Also, they administer recommended immunization such as Hepatitis B vaccinations to adults, offer advice and administer travel vaccines.
As health care gravitates more from treatment to prevention of infections, nurses have a significant role in health promotion for patients, communities, and immunization for preventive purpose. With a range of ways to promote healthy living and preventing disease, nurses should be proactive in providing education on eliminating risk factors.
NursingWritingServices.com is a reputable online platform that provides top-notch nursing writing services to students and professionals in the healthcare industry. The website is dedicated to offering high-quality academic and professional writing services to meet the unique needs of individuals seeking nursing-related help.
Discover More
Latest Samples
Contact info, company menu.
- Contacts Us
- Our Writers & Editors
- Terms of Service
- Privacy Policy
- Complaints Policy
- Fraud Policy
- Fair Use Policy
- Revision Policy
- Money Back Guarantee Policy
- Testimonials & Customer Reviews
Popular Services
- Write My Nursing Research Proposal
- Adelaide Nursing Writing Services
- Australia Nursing Writing Services
- Best Nursing Care Plan Writers
- Best Nursing Case Study Writers
- Best Nursing Dissertation Writers
- Best Nursing Essay Writers
- Best Nursing Research Paper Writers
- Best Nursing Term Paper Writers
- Best Nursing Thesis Writers
- Brisbane Nursing Writing services
- Legit Nursing Writers
- Melbourne Nursing Writing Services
- New Zealand Nursing Writing Services
- Nursing Admission Essay Writers
Nurse’s Role in Health Promotion
A significant role in maintaining and forming the principles of a healthy lifestyle and motivation to preserve health is played by medical workers, particularly nurses. It is possible to form skills for maintaining health and the need to strengthen it at the preclinical stage. A nurse should give the necessary recommendations considering age, physical development, and belonging to a particular culture.
For measures to form a healthy lifestyle of the population to bring the expected effect, it is necessary to consider the patient’s cultural specifics. The set of methodological recommendations for the organization and conduct of work with patients should differ depending on the cultural background. Methods at different levels of preventive work of the average medical staff rely on the target audience, which guarantees the effectiveness of the measures taken.
It is worth applying the Health Belief Model to each specific culture when planning patient care. For example, when conducting health education among black men, it is necessary to appeal to an increasing number of sexually transmitted infections among the black population (Plowden, 2003). Training in the prevention of diseases of the reproductive system will be of increased importance for this group of people. Therefore, the methods of organizing sanitary and hygienic education should be based on the prevention of STIs.
For measures to form a healthy lifestyle of the population to bring the expected effect, it is necessary to take cultural peculiarities into account. Prevention of diseases and promotion of a healthy lifestyle should consider the risk factors for the health of a particular ethnic group. Measures to ensure all conditions for observing a healthy lifestyle should also be selected according to the population affiliation to ensure that they can be followed.
Plowden, K. (2003). A theoretical approach to understanding black men’s health-seeking behaviour. Journal Of Theory Construction & Testing , 7(1), 27-31.
Cite this paper
- Chicago (N-B)
- Chicago (A-D)
StudyCorgi. (2022, September 16). Nurse’s Role in Health Promotion. https://studycorgi.com/nurses-role-in-health-promotion/
"Nurse’s Role in Health Promotion." StudyCorgi , 16 Sept. 2022, studycorgi.com/nurses-role-in-health-promotion/.
StudyCorgi . (2022) 'Nurse’s Role in Health Promotion'. 16 September.
1. StudyCorgi . "Nurse’s Role in Health Promotion." September 16, 2022. https://studycorgi.com/nurses-role-in-health-promotion/.
Bibliography
StudyCorgi . "Nurse’s Role in Health Promotion." September 16, 2022. https://studycorgi.com/nurses-role-in-health-promotion/.
StudyCorgi . 2022. "Nurse’s Role in Health Promotion." September 16, 2022. https://studycorgi.com/nurses-role-in-health-promotion/.
This paper, “Nurse’s Role in Health Promotion”, was written and voluntary submitted to our free essay database by a straight-A student. Please ensure you properly reference the paper if you're using it to write your assignment.
Before publication, the StudyCorgi editorial team proofread and checked the paper to make sure it meets the highest standards in terms of grammar, punctuation, style, fact accuracy, copyright issues, and inclusive language. Last updated: September 16, 2022 .
If you are the author of this paper and no longer wish to have it published on StudyCorgi, request the removal . Please use the “ Donate your paper ” form to submit an essay.
The Perceived Power and Powerlessness in School Health Nurses' Mental Health Promotion Practices: A Synthesis of Qualitative Studies
Affiliations.
- 1 Department of Health Sciences, University West, Trollhättan, Sweden.
- 2 Lindholmens Tekniska Gymnasium, The Educational Administration, City of Gothenburg, Sweden.
- 3 Children's and Adolescent's Medical Services, Region Västra Götaland, Sweden.
- PMID: 38602147
- DOI: 10.1177/10598405241241212
Schools are important arenas for mental health promotion initiatives. School nurses have the opportunity and ability to support and promote students' mental health, but their role and practices have been perceived as somewhat unclear. Therefore, the aim of this study was to explore school nurses' mental health promotion practices. A total of 12 scientific studies were synthesized through a meta-ethnographic approach. The overarching results of the synthesis show that school nurses' mental health promotion practices are largely about balancing and combining the students' needs with different professional perspectives, competencies, and conditions. The school nurses perceived that they had the power to influence their practices through a variety of ways, highlighting the importance of letting the students' needs guide the practices. Yet, at the same time they described feelings of powerlessness because of the different organizational structures that were hindering their mental health promotion practices.
Keywords: School nursing; health promotion; mental health; meta-synthesis; qualitative research.
Publication types
- Open access
- Published: 10 April 2024
Prevalence of dyslipidaemia within Polish nurses. Cross-sectional study - single and multiple linear regression models and ROC analysis
- Anna Bartosiewicz 1 ,
- Justyna Wyszyńska 1 ,
- Piotr Matłosz 2 ,
- Edyta Łuszczki 1 ,
- Łukasz Oleksy 3 &
- Artur Stolarczyk 4
BMC Public Health volume 24 , Article number: 1002 ( 2024 ) Cite this article
22 Accesses
Metrics details
Maintaining good health is vital not only for own well-being, but also to ensure high-quality patient care. The aim of this study was to evaluate the prevalence of dyslipidaemia and to determine the factors responsible for the development of this disorder among Polish nurses. Lipid profile disorders are the most prevalent and challenging risk factors for the development of cardiovascular disease. Nurses have significant potential and play a crucial role in providing care and treatment services.
This cross-sectional study involved nurses and included measurements of body weight composition (Tanita MC-980), body mass index, waist circumference, blood pressure (Welch Allyn 4200B), lipid profile, and fasting blood glucose (CardioChek PA).
The results revealed that more than half of the nurses (60.09%) were overweight or obese, with 57.28% exhibiting elevated blood pressure, 32.25% having fasting glucose levels, and 69.14% experiencing dyslipidaemia. Multiple model evaluation using ROC curves demonstrated that multiple models accurately predicted hypercholesterolemia (AUC = 0.715), elevated LDL (AUC = 0.727), and elevated TC (AUC = 0.723) among Polish nurses.
Comprehensive education programmes should be implemented that include the latest advances in cardiovascular disease prevention. Regular check-ups, as well as the promotion and availability of healthy food in hospital canteens, are essential.
Peer Review reports
Introduction
Nurses are the largest medical profession in the world, accounting for almost 60% of all medical workers in the global health sector. They have great potential and play a pivotal role in providing care and treatment services [ 1 ]. However, due to stress, overwork, high patient demands and workplace hazards, the incidence of morbidity among healthcare workers is higher compared to the general population [ 2 , 3 ]. Long shift work hours, disturbance of the natural rhythm of sleep and metabolism combined with low physical activity predispose to the development of non-communicable diseases [ 4 , 5 , 6 , 7 , 8 ].
Lipid profile disorders are the most widespread and difficult to control risk factor predisposing to the development of cardiovascular disease, the most common cause of death in the world. among nurses [ 9 – 10 ]. In combination with smoking, low physical activity, overweight, and obesity, they are the main factors in the development of atherosclerosis and its complications [ 11 , 12 ]. Taking into account data from the past five years, the life expectancy of Polish nurses is approximately 20 years less than that of the average Polish woman [ 13 ]. The median age at which nurses die is only 61.5 years, significantly less than the current median age of death for women in Poland as a whole, which is 81.8 years [ 13 ].
The data mentioned above are really alarming and indicate that the health conditions among nurses can be very poor. However, such data should be a trigger for further research on this issue. Subsequently, such research might be a basis for the implementation of non-communicable diseases prevention programmes among nurses. Prevention efforts should also address myocardial ischemia with no obstructive coronary arteries (INOCA), a chronic coronary syndrome that is recognized as a significant contributor to adverse cardiovascular outcomes, including myocardial infarction and heart failure with preserved ejection fraction. Although INOCA affects both women and men, women are more likely to be diagnosed with INOCA and experience more severe effects of angina, leading to recurrent hospitalisations and reduced quality of life. This is particularly relevant for nurses, as most of them are women [ 14 ].
This study is one of the first to do so comprehensively in Poland that evaluates parameters related to the prevalence of dyslipidaemia in this occupational group.
The purpose of the study was to evaluate the prevalence of dyslipidaemia and to determine the factors responsible for the development of this disorder among Polish nurses.
Materials and methods
The study was carried out according to the Declaration of Helsinki guidelines and was approved by the University Bioethics Commission (Resolution No. 2022/088). Before the study was started, written informed consent was obtained from nurses. No information allows respondents to be identified.
Study participants
The study was conducted in 2022 among nurses working in a randomly selected hospital in Rzeszów, after obtaining the hospital director’s consent to carry out the measurements among nurses. The project has also been approved by the head of nurses. In consultation with hospital authorities, the information included dates, hours, and the scope of the planned examinations for the attention of all nurses working on individual hospital wards. Nurses willing to participate in the study could sign up on the prepared list and choose a convenient date. All measurements (body mass analysis, glucose level, lipid profile) were performed in the morning from 7.00 to 10.00 a.m., at least 8 h of fasting. Participation in the study was voluntary and free. The following recruitment criteria were used: professionally active nurses, with no infection symptoms within the last 2 weeks, unaware of health problems, not undergoing treatment for the aforementioned conditions or medical nutritional therapy, and willing to participate in the project. Data from the measurements of 405 nurses were subjected to statistical analysis.
Measurement
All measurements were carried out took place in the following order: signing an individual consent to participate in the study, 10 min of rest, completing a questionnaire, blood pressure measurement, glucose and lipid profile measurement, anthropometric measurements, and body composition analysis.
Blood pressure (BP) measurement
Systolic blood pressure (SBP) and diastolic blood pressure (DBP) were measured after a 10 min rest in the sitting position with the back supported and the feet on the floor. Measurements were made in the right arm with the elbow placed at heart level using a cuff adjusted to the arm circumference of the subjects. A Welch Allyn 4200B apparatus (Aston Abbotts, UK) was used for the measurements. Measurements were made three times according to the guidelines of experts of the European Society of Hypertension [ 14 ]. The average of three measurements was calculated for each participant.
The following cutoff criteria were used:
Normal blood pressure: 120–129 mmHg / 80–84 mmHg,
Normal high pressure: 130–139 mmHg / 85–89 mmHg,
Grade 1 hypertension: 140–159 mmHg / 90–99 mmHg,
Grade 2 hypertension: 160–179 mmHg / 100–109 mmHg,
Grade 3 hypertension: ≥ 180 mmHg / ≥ 110 mmHg [ 15 ].
Body composition measurement
Body composition was measured by bioelectric impedance (6.25 kHz, 50 kHz, 90 µA) using a certified and calibrated analyzer (Tanita MC-980 PLUS MA, Tokyo, Japan) with an accuracy of 0.1 kg/0.1%. The analyzer has 8 electrodes (4 built in the platform and 4 in the holders). To ensure accurate measurements, the device was placed on a level surface according to the instructions, in such a way as to ensure that the level indicator is centered on the level meter. The participants entered the analyzer platform barefoot, in light clothing, in an upright position, motionless, placing their feet in a way that ensured an even distribution of body weight and contact with the electrodes. Measurement was carried out in a standing position, contact with the electrodes was provided by bare feet and hands held away from the body at an angle of 35°-40°. The Tanita software automatically measured body mass and impedance to determine the percentage of body fat, based on formulas and equations that are generalized to standard adults. The Tanita MC 980 device has approvals for medical use and meets the NAWI and CLASS III standards and the MDD 93/42/EEC directive, as well as the CE0122 EU certificate [ 16 ].
Anthropometric measurement
Anthropometric measurements were measured using an anthropometric tape according to the ISAK protocol (The International Society of the Advancement of Kinanthropometry) by a member of the ISAK Level 3 accredited research team, a full profile anthropometrist technician. Body height was measured with an accuracy of 0.1 cm using a Seca 213 stadiometer. The measurements were made under standard conditions, barefoot in an upright position. The mean value of three measurements was used in the analyses.
Waist hip ratio (WHR)
The following normative ranges were adopted for the value of the WHR index:
< 0.96 WHR within normal limits
≥ 0.96 Abdominal obesity, increased risk of metabolic diseases.
< 0.83 WHR within normal limits
≥ 0.83 Abdominal obesity, increased risk of metabolic diseases [ 17 ].
Waist-to-height ratio (WHtR)
The following normative ranges were adopted for the value of the WHtR index:
Men and women:
< 0.5 value of the index within normal limits
0.5–0.6 increased cardiometabolic risk
≥ 0.6 significantly increased cardiometabolic risk [ 18 ].
Body mass index (BMI)
BMI was calculated automatically by the Tanita MC-980 MA body composition analyzer Tanita MC-980 MA) as body weight (kg)/height (m) 2 . Criteria of body mass deficiency, normal body weight, overweight, and obesity recommended by the Centers for Disease Control and Prevention were used [ 19 ].
The following cut-off criteria of Body Mass Index were adopted:
17–18.49 = underweight,
18.5–24.99 = normal body weight,
25–29.99 = overweight,
30–34.99 = 1st degree.
35–39.99 = 2nd degree obesity,
> 40 = 3rd degree obesity [ 19 ].
Laboratory tests
A finger prick capillary whole blood sample was collected from each nurse and analysed using the CardioChek PA (CCPA) analyzer according to the manufacturer’s instructions. Capillary samples were collected by a registered nurse, observing all the rules of asepsis and antisepsis.
Using the collection device supplied with the CCPA that was compatible with the CardioChek reagent test strips (35–40 µL sample volume). Blood samples were collected in the morning after a fast of 9–12 h of the night. Total cholesterol (TC), low-density lipoprotein (LDL), high-density lipoprotein (HDL), triglycerides (TG), and glucose levels were evalueted. The CCPA device was checked each time before starting by Internal Quality Control using a control strip recommended by the manufacturer. Maintenance was performed according to the manufacturer’s instructions [ 20 , 21 ].
Dyslipidemia cut point criteria
Hypercholesterolemia was diagnosed when TC was ≥ 190 mg/dL or LDL > 115 mg/dL. Atherogenic dyslipidemia was determined when TG was ≥ 150 mg/dL, HDL < 40 mg/dL in males and < 48 mg/dL in females, and elevated LDL fraction (> 130 mg/dl).
Hypertriglyceridemia was determined when TG was > 150 mg/dL with normal LDL levels (< 115 mg/dl) and severe hypertriglyceridemia - TG ≥ 800 mg/dL [ 22 , 23 ].
Lipid profile cut point criteria
TC: 150–190 mg/dl.
LDL cholesterol: less than 115 mg/dl.
HDL cholesterol: men above 40 mg/dl, women over 48 mg/dl,
TRG: below 150 mg/dL [ 24 ].
Fasting glucose cut point criteria
Less than 70 mg / dl - hypoglycemia,
70 to 99 mg/dL - normal glucose level,
100 to 125 mg/dL - elevated glucose levels - pre-diabetes,
≥ 126 mg/dL at least two measurements - diabetes mellitus [ 25 ].
Furthermore, based on the results of the lipid profile the atherogenicity indicators are determined, e.g. Castelli index (TC/HDL), LDL/HDL ratio, and TG/HDL ratio. Elevated values of these indicators demonstrate the risk of developing atherosclerosis, ischemic heart disease, or stroke, and indicate the need to immediately change eating habits and/or pharmacotherapy.
Atherogenicity indicators cut points
TC/HDL: men: <4.5; women: <4.0,
LDL/HDL ratio - the correct result should be 1:3 − 1:2.
TG/HDL ratio: the optimal score is < 2, which means that we have mainly large LDL lipoprotein particles, and therefore harmless to our health. A score > 2 means a high risk of developing cardiovascular disease due to the predominance of mainly small and dense LDL particles [ 22 , 26 ].
Questionnaires
The questionnaire package was prepared in paper form with an attached envelope, allowing the completed questionnaires to be sealed, and thus ensuring the confidentiality of the responses provided. The survey included questions about the sociodemographic data of the respondents including age, gender, place of work, type of work, and educational level (basic, bachelor’s, and master’s). Additional questions were related to the most frequently consumed groups of food products, salt intake, participation in preventive examinations, weight control, smoking (the response ‘yes’ indicates individuals who smoked regularly in the past as well as those who currently smoke, the response ‘no’ indicates that the person does not currently smoke and has not smoked in the past), work system, self-assessment of health condition.
Quality Control
To ensure the high quality of the research conducted, a research strategy was developed. A four-person team of university employees consisting of a nurse, dietician, physiotherapist, and full profile anthropometrist technician were responsible for supervising the measurements, directing study participants to the appropriate measurement stations, collecting questionnaires, and coding the obtained results. The research survey and raw measurement data have been double-checked to ensure the authenticity and accuracy of the data, including effective data logic checks, and editing checks. To protect the personal data of the participants and ensure the confidentiality of these data, each nurse was assigned as an individual ID number, developed according to a previously adopted algorithm, which was used during the measurements, results processing, processing, and statistical analysis of the data. The database was built using Excel and data was entered twice by two data managers to ensure accuracy and integration.
Statistical analysis
The analysis was performed using R programme, version 4.2.1 [ 27 ]. The analysis of quantitative variables (i.e. expressed in numbers) was performed by calculating the average, standard deviation, median, and quartiles. The analysis of qualitative variables (i.e. not expressed in numbers) was performed by calculating the number and percentage of occurrences of each value. A single and multiple analysis of the influence of many variables on a binary variable (presence or absence of hypercholesterolemia) was performed using logistic regression. Results are presented as values of odds ratio (OR) parameters with a 95% confidence interval. The variables for the multiple analysis was selected on the basis of their significance in the one-factor analyses. The EPV (events per variable) index for the analysis was 8.7. The quality of the multiple models were assessed using the ROC (Receiver operating characteristic) curves and the areas under curve (AUC). The analysis adopted a significance level of 0.05. Thus, all p-values below 0.05 were interpreted as significant associations.
Characteristics of the study group
In total, 405 nurses participated in the measurements, the vast majority of the participants ( n = 380; 93.83%) were women. The average age of the respondents was approximately 48.5 years (SD ± 10.44). Detailed characteristics of the study group are presented in Table 1 .
The declaration of daily consumption of specific food product groups is as follows: white bread 56.3%, dark bread 25.43%, fish and seafood 1.73%, red meat and sausages 19.26%, sour milk products 27.9%, cheese 25.19%, cottage cheese 22.22%, fruits and vegeTable 70.12%, sweets and salty snacks 27.41%, fast food products 4.69%. The exact frequency of consumption of selected groups of food products is presented in Table 2 .
The results of BMI, WHR, WHtR, blood glucose, body fat percentage (BFP), visceral fat index (VFI), total body water and phase angle are shown in Table 3 .
The results showed that more than half of the nurses participating in the measurements ( n = 249; 61.48%) had hypercholesterolemia. Severe hypertriglyceridemia has not been reported. The occurrence of individual forms of dyslipidemia in the study group is presented in Table 4 .
Single-factor logistic regression models (separate for each of the analyzed features) showed that significant predictors (p<0.05) of the risk of developing hypercholesterolemia are age (OR = 0.058), participation in preventive examinations other than obligatory (OR = 1.834), obesity and BMI grade (OR = 3.096), WHR abdominal obesity (OR = 2.135), WHtR increased cardiometabolic risk (OR = 1.969), WHtR significantly increased cardiometabolic risk (OR = 2.117), SBP (OR = 1.012), hypertension Stage I (OR = 1.888), stage II hypertension (OR = 15.573), increased body fat (OR = 1.641), excessive body fat (OR = 3.199), low body water (OR = 2.085). The multiple logistic regression model showed that age (OR = 1.038) and grade II hypertension (OR = 12.589) are significant (p<0.05) independent predictors of the risk of developing hypercholesterolemia (details available in supplementary materials - Table S1 ).
The quality of the multidimensional models was assessed using the receiver operating characteristic (ROC) curves and the areas below them. The area under curve (AUC) for the multiple models was 0.715. Therefore, the multiple model predicts the occurrence of hypercholesterolemia quite well (Fig. 1 ).

ROC curve and AUC value for hypercholesterolaemia
Single-factor logistic regression models (separate for each of the analyzed features) showed that significant (p<0.05) predictors of the risk of developing elevated LDL are: age (OR = 1.052), higher education (OR = 0.572), participation in preventive examinations other than obligatory (OR = 1.999), consumption of fish and seafood several times a month (OR = 0.517), consumption of fast food products (OR = 0.584), 1st degree obesity according to BMI (OR = 2.595), abdominal obesity according to WHR (OR = 2.354), increased cardiometabolic risk by WHtR (OR = 2.078), significantly increased cardiometabolic risk by WHtR (OR = 2.392), SBP (OR = 1.012), grade I hypertension (OR = 2.405), grade II hypertension (OR = 2.354), = 6.328), excessive body fat (OR = 3.435) and low body water content (OR = 2.299). The multiple logistic regression model showed that significant independent predictors (p<0.05) of the risk of developing elevated LDL are: participation in prophylactic examinations other than obligatory (OR = 1.792), consumption of fish and seafood several times a month (OR = 0.514), consumption of fast food products (OR = 0.59), abdominal obesity according to WHR (OR = 1.748), 1st degree hypertension (OR = 2.632), 2nd degree hypertension (OR = 7.096), (details available in supplementary materials - Table S2 ).
The area under curve (AUC) for the multiple models was 0.727. The multiple model predicts the occurrence of an elevated low-density lipoprotein (LDL) level in the study group quite well (Fig. 2 ).

ROC curve and AUC value for LDL
Logistic regression models (separate for each of the analyzed characteristics) showed that significant (p<0.05) predictors of the risk of developing elevated TC are: male gender (OR = 0.363), age (OR = 1.061), participation in preventive examinations other than obligatory (OR = 1.855), 1st degree obesity according to BMI (OR = 2.595), abdominal obesity according to WHR (OR = 2.047), increased cardiometabolic risk according to WHtR (OR = 1.895), SBP (OR = 1.012), 1st degree hypertension ( OR = 1.864), grade II hypertension (OR = 11.043), excessive body fat (OR = 2.352) and low body water (OR = 1.853). The multiple logistic regression model showed that significant (p<0.05) independent predictors of the risk of elevated TC are male gender (OR = 0.279), age (OR = 1.042) and grade II hypertension: OR = 11.487), (details available in supplementary materials - table S3 ).
The area under curve (AUC) for the multiple models was 0.723. Therefore, the multiple model predicts the occurrence of an elevated total cholesterol (TC) level quite well (Fig. 3 ).

ROC curve and AUC value for TC
To our knowledge, this is the first study to evaluate the prevalence of individual components of dyslipidaemia and to determine the factors responsible for the development of this disorder in the nursing population. Most of the nurses who participated in the measurements had lipid profile disorders ( N = 280; 69.14%), elevated blood pressure ( N = 232; 57.28%), increased body weight ( N = 231; 57.03%) and 31% had elevated glucose levels.
Most studies are related to patients, but few assess the health of healthcare professionals providing comprehensive health care [ 2 ]. According to the WHO, only half of countries in the world have health profiles of their employees, unfortunately, noncommunicable diseases and those related to lifestyle are not taken into account to the least extent [ 28 ]. Due to the overload of work and the growing demands of patients and employers, healthcare professionals pay little attention to their personal well-being and health [ 29 ]. Taking into account the data of the last five years, the median age of death for nurses is only 61.5 years, which is much lower than the current median age of death for Polish women overall, which is 81.8 years [ 13 ]. The study conducted on a population of thousands of people over 15 years has shown that the health condition of healthcare workers is much worse compared to the general population. Researchers based on large national medical history data sets have also shown that the percentage of deaths among physicians and nurses is much higher [ 30 ]. The specificity of the work environment of nurses is the cause of physical and biological hazards, violence, and loads on the musculoskeletal system. Furthermore, shift work and the resulting disturbances in the natural rhythm of sleep, rest, regular meals, and lack of time for physical activity predispose to the development of many metabolic diseases [ 31 , 32 , 33 ].
Our research has shown that more than half (56.3%) of nurses declared daily consumption of white bread. Sweets/salty snacks and cheese are eaten daily by more than a quarter of nurses, and red meat and its products, as well as fast food products, are eaten by almost 20% of the nurses surveyed. Furthermore, the respondents declare a relatively low consumption of fish and seafood; only a small percentage of the respondents (0.74%) do not include fruits and vegetables in their daily diet. The insufficient consumption of these products is indicated by the results of a study conducted among nurses in Delhi [ 34 ]. Results Nora et al. showed that the factor that affected the consumption of certain product groups and the deterioration of eating habits was stress at work or work under onerous circumstances. According to the researchers, nurses who worked with COVID-19 patients ate significantly less fruit and vegetables. Additionally, up to 76.2% of nurses declared financial difficulties in buying healthy food [ 35 ]. In another study, most nurses indicated that it is difficult to maintain proper eating habits at work, because the food they often receive from patients as a gift contains a lot of sugar and fat and is easily available [ 36 , 37 ]. In the study by Wojcza et al. almost all nurses (94.5%) included in the survey declared bad eating habits, especially nurses who were overweight/obese and declared additional employment [ 38 ].
Our measurements showed that more than half of nurses (60.09%) were overweight and/or obese. Furthermore, the values of the WHR and WHtR indices in almost half of the subjects indicated the presence of abdominal obesity and increased cardiometabolic risk. The results of measurements made using a body composition analyser showed that 42.47% had increased or excessive body fat. Many studies confirm that the occurrence of overweight and obesity among nurses is quite common. A Scottish cross-sectional study showed that obesity among nurses is more common not only in relation to the general population, but also among other healthcare professionals [ 39 , 40 ]. A similar trend is also observed in Great Britain, New Zealand, the United States, and Australia [ 41 , 42 ]. In a study by Kayaroganam et al., evaluating the profiles of noncommunicable disease risk factors among nurses in a tertiary care hospital in South India, more than two-thirds of nurses had abdominal obesity (71.6%), more than half were obese (57.2%), and one fifth were overweight (20.5%), mainly women over 40 years of age [ 12 ].
In our study, a total of 57.28% of nurses had elevated blood pressure and hypertension of the first and second degree. Furthermore, a total of 32.25% of the subjects had glucose abnormalities, most of which were related to elevated glucose levels. Hypertension is a global problem and the leading cause of morbidity and premature death [ 43 ]. In the Manakali study, 52% of nurses had hypertension, significantly higher than the reported prevalence of hypertension among nurses in South Africa (20%), Brazil (32%) and healthcare professionals in Nigeria (20.1%). This result is also higher than the documented prevalence of hypertension in the general adult population of South Africa [ 44 , 45 , 46 , 47 ]. In the Kayaroganam study, about a quarter of nurses had elevated BP (14.4%) and elevated blood glucose (11.5%) [ 39 ]. Some studies indicate that elevated glucose levels among nurses may also be the result of stress experienced at their daily work [ 48 , 49 ].
Dyslipidaemia occurred in 69.14% of nurses who participated in the measurements and was most often related to hypercholesterolemia (61.48%). There was also an increased level of atherogenicity indexes, especially in the case of the TG/HDL index. Dyslipidaemia predisposes to the development of cardiovascular diseases, atherosclerosis, and, consequently, to ischemic heart disease and stroke [ 50 ]. The results of a study conducted in South India showed that more than one-third of nurses had hypercholesterolemia (34.3%) and elevated LDL (41.9%) and two-thirds had low HDL (65.3%). Hypercholesterolemia and triglyceridemia were significantly higher among men and those who were married. Elevated LDL levels were significantly higher among men and people < 50 years of age, while low HDL levels were significantly higher among women 30 to 39 years of age [ 39 ]. Researchers from Ghana observed that an increase in glycemia was associated with a corresponding increase in atherogenic lipid parameters. Among nurses with atherogenic dyslipidaemia (26.29%), there were also numerous lipid abnormalities. A significant additive trend was observed between the mean markers of atherogenic dyslipidaemia and the degree of obesity. In all cases, the levels of atherogenic markers of dyslipidaemia increased from underweight and reached peak at overweight or obesity [ 51 ]. Regression analysis showed that significant predictors ( p < 0.05) of the risk of developing hypercholesterolemia in the one-factor model are age, participation in preventive examinations other than obligatory, obesity of the first degree, abdominal obesity, increased and significantly increased cardiometabolic risk, SBP, hypertension of the first and second degree, increased and excessive body fat and low body water content. In the case of the risk of developing elevated LDL, education, rare consumption of fish and seafood, and consumption of fast-food products are also important predictors, while in the case of elevated TC, male gender. Significant independent predictors (p<0.05) of the risk of hypercholesterolemia in the multiple models are age and grade II hypertension, in the case of LDL, in addition to those listed, participation in preventive examinations, rare fish consumption, fast food consumption, abdominal obesity and grade I and II hypertension. However, in the case of the risk of elevated TC, male sex, age, and grade II hypertension. Hojat et al. analysing risk factors for cardiovascular diseases among male and female nurses showed that there was a statistically significant difference between women and men in indicators such as eating breakfast, family history, fruit consumption, high-density lipoprotein (HDL), BMI, and WHR [ 52 ]. Whereas in study by Gadallah et al., the only predictor of high LDL was age ≥ 40 years, whereas unhealthy diet and night shift work were predictors of risky HDL levels [ 53 ].
The nature of nurses’ work predisposes them to many health problems. Shift work and disrupting the natural rhythm of sleep, rest and regularity of eating meals are the cause of overweight, obesity, hypertension, dyslipidaemia, and, consequently, cardiovascular diseases. A study by the Cardiovascular Nurses Association showed that hypertension, heart disease, and dyslipidaemia are common among nurses [ 54 ]. Health professionals are an important resource for each country [ 55 ]. Taking care of your health, you can be good models for your patients, families, and friends [ 56 ]. The Galen, one of the most eminent ancient physicians, has said: “The physician will hardly be thought very careful of the health of his patients if he neglects his own”. It should be taken into account for creating solutions at the government and institutional level, limiting risk factors for progression dyslipidaemia among nurses [ 2 ].
Strengths, limitations, and future research
To our knowledge, this is one of the first such comprehensive studies in Poland to assess parameters related to the prevalence of dyslipidaemia in this occupational group. There are also several potential study limitations that should be considered when interpreting the results. This study had a limited geographic scope and should be extended to more medical facilities in other regions. Since the study is cross-sectional, causality and temporality issues should not be considered. More research is needed in a larger population across all age groups.
Conclusions
The study showed that the prevalence of disorders of the lipid profile in the study group is high, especially hypercholesterolemia. Nurses declared bad eating habits, which could be the cause of obesity, overweight, elevated glucose levels, and hypertension. The evaluation of multiple models using ROC curves showed that the multiple models predict hypercholesterolemia (AUC = 0.715), elevated LDL (AUC = 0.727) and elevated TC (AUC = 0.723) quite well among the nurses surveyed. Our study shows most of the risk factors among the nursing population in the Subcarpathian region of Poland. The possession of medical knowledge and access to medical entities do not protect nurses against the risk of diseases. Broadly understood education should be implemented, including the latest trends in the prevention of cardiovascular disease. Regular check-ups and the promotion and availability of healthy food in hospital canteens are necessary.
The practical implications for non-communicable disease prevention
Bearing in mind obtained results and literature review as well as considering the importance of prevention non-communicable diseases among nurses, the following recommendations could be included:
Dietary modifications may involve recommendations to replace salt with potassium chloride and herbs, as well as eliminating the consumption of high-calorie and highly processed products. Particularly recommended are the Dietary Approaches to Stop Hypertension (DASH) diet for the prevention and treatment of hypertension, and the Mediterranean diet, which presents not only a way of nutrition but also a holistic model of a healthy lifestyle [ 57 , 58 , 59 ].
Another important issue for improvement of nurses’ health conditions is engaging in physical activity beyond the scope of daily nursing duties. Here, with the support of employers, it is worth promoting exercise programs that encourage and facilitate physical activity [ 60 , 61 ].
For nurses at increased cardiovascular risk, it is crucial to consider the potential benefits of statin therapy, as recommended by reputable sources for individuals with elevated cardiovascular risk. This is particularly important for individuals for whom lifestyle modifications are challenging or ineffective. Offering guidance on the appropriate use of statins could assist in preventing cardiovascular diseases among nurses [ 62 ].
It is also important to leverage expertise from multiple stakeholders in order to drive transformational change in building safe, secure and responsive healthcare working environments [ 63 ]. By incorporating these recommendations into the documents, can provide comprehensive guidance on health preventive among nurses, addressing the reviewer’s feedback effectively. The present study emphasizes on behavior change campaign among health professionals to motivate them to adopt healthy lifestyle and prevention of non-communicable diseases. Moreover, nurses who know their risk factors and who follow healthy lifestyle behaviors will be more effective in counseling roles for patients.
Data availability
The dataset supporting the conclusions of this article is included within the article (and its additional file).
World Health Organization (WHO). State of world’s nursing 2020: Investing in Education, Jobs and Leadership. WHO, Geneva. 2020. Retrieved from: https://www.who.int/publications/i/item/9789240003279 . Accessed on 20 September 2022).
Mohanty A, Kabi A, Mohanty AP. Health problems in healthcare workers: a review. J Fam Med Prim Care. 2019;8:2568.
Article Google Scholar
Huang HL, Pan CC, Wang SM, et al. The incidence risk of type 2 diabetes mellitus in female nurses: a nationwide matched cohort study. BMC Public Health. 2016;16:443.
Article PubMed PubMed Central Google Scholar
Bartosiewicz A, Łuszczki E, Nagórska M, Oleksy Ł, Stolarczyk A, Dereń K. Risk factors of metabolic syndrome among Polish nurses. Metabolites. 2021;11:267.
Article CAS PubMed PubMed Central Google Scholar
Domingues JG, Silva BB, Bierhals IO, Barros FC. Noncommunicable diseases among nursing professionals at a charitable hospital in Southern Brazil. Epidemiol Serv Saude. 2019;28. https://doi.org/10.5123/S1679-49742019000200011 .
Sharma D, Vatsa M, Lakshmy R, Narang R, Bahl VK, Gupta SK. Study of cardiovascular risk factors among tertiary hospital employees and their families. Indian Heart J. 2011;63:418–24.
PubMed Google Scholar
Dutheil F, Baker JS, Mermillod M, De Cesare M, Vidal A, Moustafa F, Pereira B, Navel V. Shift work, and particularly permanent night shifts, promote dyslipidaemia: a systematic review and meta-analysis. Atherosclerosis. 2020;313:156–69.
Article CAS PubMed Google Scholar
Sooriyaarachchi P, Jayawardena R, Pavey T, King NA. Shift work and the risk for metabolic syndrome among healthcare workers: A systematic review and meta-analysis. Ob. Rev.2022; 23: e13489. https://onlinelibrary.wiley.com/doi/full/10.1111/obr.13489 . (Accessed on 10 May 2023).
Soppert J, Lehrke M, Marx N, Jankowski J, Noels H. Lipoproteins and lipids in cardiovascular disease: from mechanistic insights to therapeutic targeting. Adv Drug Deliv Rev. 2020;1:4–33.
Yao YS, Li TD, Zeng ZH. Mechanisms underlying direct actions of hyperlipidemia on myocardium: an updated review. Lipids Health Dis. 2020;19:23.
Després JP. Body fat distribution and risk of cardiovascular disease: an update. Circulation. 2012;4:1301–13.
Kayaroganam R, Sarkar S, Satheesh S, Tamilmani S, Sivanantham P, Kar SS. Profile of non-communicable disease risk factors among nurses in a tertiary care hospital in South India. Asian Nurs Res. 2022;1:241–8.
Main Chamber of Nurses and Midwifes in Poland. Report: Nurse, midwife, shortage professions in the Polish health care system. Retrieved from: https://nipip.pl/wp-content/uploads/2022/06/2022_Raport-NIPiP-struktura-wiekowa-kadr.pdf . Accessed on 22 September 2022).
Mehta PK, Huang J, Levit RD, Malas W, Waheed N, Bairey Merz CN. Ischemia and no obstructive coronary arteries (INOCA): a narrative review. Atherosclerosis. 2022;12:363:8–21. https://doi.org/10.1016/j.atherosclerosis.2022.11.009 .
Article CAS Google Scholar
Williams BR, Mancia G, Spiering W, Rosei E, Azizi M, Burnier M, Clement DL, Coca A, de Simone G, Dominiczak A, Kahan T. ESC/ESH guidelines for the management of arterial hypertension. Kardiologia Polska (Polish Heart Journal). 2019;77:71–159.
Article PubMed Google Scholar
Tanita. November. Professional Product. Guide. https://tanita.eu/media/wysiwyg/catalogue/tanita_pro_product-guide_april_2017.pdf (12 2022).
Nishida C, Ko G, Kumanyika S. Body fat distribution and noncommunicable diseases in populations: overview of the 2008 WHO Expert Consultation on Waist Circumference and Waist–hip ratio. Eur J Clin Nutr. 2010;64:2–5.
Gibson S, Ashwell M. A simple cut-off for waist-to-height ratio (0·5) can act as an indicator for cardiometabolic risk: recent data from adults in the Health Survey for England. Br J Nutr. 2020;123:681–90.
Barlow SE. Expert Committee. Expert committee recommendations regarding the prevention, assessment, and treatment of child and adolescent overweight and obesity: summary report. Pediatrics. 2007;120:164–92.
PTS Diagnostics. User guide. CardioCheck PA Test System. https://ptsdiagnostics.com/wp-content/uploads/2018/09/ps-002461-en_rev._4_user_guide_cardiochek_pa.pdf . (Accessed on 14 October 2022).
Gao Y, Zhu CG, Wu Q, Guo L, Liu G, Dong Q, Li JJ. Study on the reliability of CardioChek PA for measuring lipid profile. J Peking Univ Health Sci. 2016;48:523–8.
CAS Google Scholar
Polish Society of Cardiology - Guidelines. Available online: https://ptkardio.pl/ (accessed on 16 December 2021).
Szymański FM, Barylski M, Cybulska B, Wożakowska-Kapłon B, Krasiński Z, Mamcarz A, Widecka K, Płatek AE, Dudek D, Mickiewicz A, Kobayashi A. Recommendation for the management of dyslipidemia in Poland—third declaration of Sopot. Interdisciplinary expert position statement endorsed by the Polish Cardiac Society working group on cardiovascular pharmacotherapy. Cardiol J. 2018;25(6):655–65.
Banach M, Burchardt P, Chlebus K, Dobrowolski P, Dudek D, Dyrbuś K, Gąsior M, Jankowski P, Jóźwiak J, Kłosiewicz-Latoszek L, Kowalska I, Wytyczne PTL/KLRWP/PTK/. Nadciśnienie Tętnicze w Praktyce. 2021;7(3):113–22. PTDL/PTD/PTNT diagnostyki i leczenia zaburzeń lipidowych w Polsce 2021.
Google Scholar
American Diabetes Association. 2. Classification and diagnosis of diabetes: standards of medical care in diabetes—2021. Diabetes care. 2021;44(Supplement_1):S15-33.
Alberti KG, Eckel RH, Grundy SM, Zimmet PZ, Cleeman JI, Donato KA, Fruchart JC, James WPT, Loria CM, Smith SCJ, et al. Harmonizing the metabolic syndrome: a joint interim statement of the international diabetes federation task force on epidemiology and prevention; national heart, lung, and blood institute; American heart association; world heart federation; international atherosclerosis society; and international association for the study of obesity. Circulation. 2009;120:1640–5.
R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Italy. 2018; Available online: https://www.R-project.org (accessed 12 November 2021).
World Health Organization. WHO Global Plan of Action on Workers’ Health (2008–2017) baseline for implementation: global country survey 2008. World Health Organization. 2013. https://www.who.int/publications/i/item/WHO-FWC-PHE-2013-01 . (Available on: 10 May 2023).
Shin Y, Kim UJ, Lee HA, Choi EJ, Park HJ, Ahn HS, Park H. Health and Mortality in Korean Healthcare Workers. J Kored Sci. 2022;17(3):37.
Azizoğlu F, Köse A, Gül H. Self-reported environmental health risks of nurses working in hospital surgical units. Int Nurs Rev. 2019;66:87–93.
Gajewska K, Sienkiewicz Z. Th einfluence of working conditions on the health of nurses working in surgical wards. Pielęgniarstwo w anestezjologii i intensywnej terapii (Nursing in anesthesiology and intensive care)2018; 4: 9–17. http://evereth.home.pl/archiwum-pdf/PAIO/2018/1/3.pdf Accessed on 08.01.2023.
Samur M, Seren IS. Nurses’ view of their work environment, health, and safety: a qualitative study. J Nur Manag. 2019;27:1400–8.
Rosa D, Terzoni S, Dellafiore F, Destrebecq A. Systematic review of shift work and nurses’ health. Occup Med. 2019;69(4):237–43.
Sharma D, Vatsa M, Lakshmy R, Narang R, Bahl VK, Gupta SK. Study of cardiovascular risk factors among tertiary hospital employees and their families. Indian Heart J. 2011;1:418–24.
Nohra RG, Naim E, Chaaban T, et al. Nurses’ eating habits in Lebanon during the economic and health crises: a cross-sectional study. Arch Public Health. 2022;80:28.
Monaghan T, et al. Factors influencing the Eating practices of Hospital nurses during their shifts. Workplace Health Saf. 2018;66:331–42.
De Lucia F, Cocchiara R, La Torre G. A systematic review of nurses’ eating habits on duty for a healthy workplace. Senses Sci. 2021;13(2):8.
Gieniusz-Wojczyk L, Dąbek J, Kulik H. Nutrition habits of Polish nurses: an Approach. Healthcare. 2021;9:786.
Kyle RG, Neall RA, Atherton IM. Prevalence of overweight and obesity among nurses in Scotland: a cross-sectional study using the Scottish Health Survey. Int J Nurs Stud. 2016;53:126–33.
Kyle RG. Prevalence of overweight and obesity among nurses in Scotland: a crosssectional study using the Scottish health survey. BMJ Open. 2016;53:126–33.
Bogossian FE, Hepworth J, Leong GM, Flaws DF, Gibbons KS, Benefer CA, Turner CT. A cross-sectional analysis of patterns of obesity in a cohort of working nurses and midwives in Australia, New Zealand, and the United Kingdom. Int J Nurs Stud. 2012;49:727–38.
Chin DL, Nam S, Lee SJ. Occupational factors associated with obesity and leisure-time physical activity among nurses: a cross sectional study. Int J Nurs Stud. 2016;57:60–9.
NCD Risk Factor Collaboration. Worldwide trends in hypertension prevalence and progress in treatment and control from 1990 to 2019: a pooled analysis of 1201 population- representative studies with 104 million participants. Lancet. 2021;11(10304):957–80.
Monakali S, Goon DT, Seekoe E, Owolabi EO. Prevalence, awareness, control, and determinants of hypertension among primary health care professional nurses in Eastern Cape, South Africa. Afr J Prim Health Care Fam Med. 2018;10:1–5.
Day C, Groenewald P, Laubscher R, Chaudhry S, van Schaik N, Bradshaw D. Monitoring of non-communicable diseases such as hypertension in South Africa: challenges for the post-2015 global development agenda. S Afr Med J. 2014;104:680–7.
Peer N, Steyn K, Lombard C, Gwebushe N, Levittet N. A high burden of hypertension in the urban black population of Cape Town: the cardiovascular risk in Black South africans (CRIBSA) study. PLoS ONE. 2013;8:e78567.
Owolabi EO, Goon D, Adeniyi OV, Seekoe E. Social epidemiology of hypertension in Buffalo City Metropolitan Municipality (BCMM): cross-sectional study of determinants of prevalence, awareness, treatment, and control among South African adults. BMJ Open. 2017;7:e014349.
Hilliard ME, Yi-Frazier JP, Hessler D, Butler AM, Anderson BJ, Jaser S. Stress and A1c among people with diabetes across the Lifespan. Curr Diab Rep. 2016;16:1–10.
Li L, Li X, Zhou W, Messina JL. Acute psychological stress results in the rapid development of insulin resistance. J Endocrinol. 2013;217:175–84.
Borén J, Taskinen MR, Björnson E, Packard CJ. Metabolism of triglyceride-rich lipoproteins in health and dyslipidaemia. Nat Rev Cardiol. 2022;19:577–92.
Osei-Yeboah J, Kye-Amoah KK, Owiredu WK, Lokpo SY, Esson J, Bella Johnson, Amoah P, Asumbasiya Aduko R. Cardiometabolic risk factors among healthcare workers: a cross-sectional study at the Sefwi-Wiawso Municipal Hospital, Ghana. BioMed Res Int. 2018;23:2018.
Hojat M, Jahromi M, Koshkaki SR, Rahmanian M. Comparison of risk factors of cardiovascular diseases in male and female nurses. J Educ Health Promot. 2019;8:1.
Gadallah M, Hakim SA, Mohsen A, Eldin WS. Association of rotating night shift with lipid profile among nurses in an Egyptian tertiary university hospital. East Mediterr Health J. 2017;14:295–302.
Fair JM, Gulanick M, Braun LT. Cardiovascular risk factors and lifestyle habits among preventive cardiovascular nurses. J Cardiovasc Nurs. 2009;240:277–86.
GBD 2019 Human Resources for Health Collaborators. Measuring the availability of human resources for health and its relationship to universal health coverage for 204 countries and territories from 1990 to 2019: a systematic analysis for the global burden of Disease Study 2019. Lancet. 2022;4(10341):2129–54.
Dunphy LM. 2005. Florence Nightingale’s 13 formal letters to her nurses (1872–1900). In: Dossey BM, Selander L, Beck, D, Attewell A. eds. Florence Nightingale Today: Healing Leadership Global Action. MD: Amer. Nurs. Assoc. Silver Spring 2005; 29–63.
Nissaisorakarn V, Ormseth G, Earle W, Morales-Alvarez MC, Hiremath S, Juraschek SP. Less sodium, more potassium, or both: population-wide strategies to prevent hypertension. Am J Physiol Ren Physiol. 2023;1(1):F99–104. https://doi.org/10.1152/ajprenal.00007.2023 . Epub 2023 Jun 1. PMID: 37262087.
Dominguez LJ, Di Bella G, Veronese N, Barbagallo M. Impact of Mediterranean Diet on Chronic Non-communicable diseases and Longevity. Nutrients. 2021;12(6):2028. https://doi.org/10.3390/nu13062028 . PMID: 34204683; PMCID: PMC823159.
Filippou C, Tatakis F, Polyzos D, Manta E, Thomopoulos C, Nihoyannopoulos P, Tousoulis D, Tsioufis K. Overview of salt restriction in the Dietary Approaches to Stop Hypertension (DASH) and the Mediterranean diet for blood pressure reduction. Rev Cardiovasc Med. 2022; 19;23(1):36. https://doi.org/10.31083/j.rcm2301036 . PMID: 35092228.
Warburton DE, Bredin SS. Health benefits of physical activity: a systematic review of current systematic reviews. Curr Opin Cardiol. 2017;1(5):541–56.
Warburton DER, Bredin SSD. Lost in translation: what does the physical activity and health evidence actually tell us? In: Zibadi S, Watson RR, editors. Lifestyle in Heart Health and Disease. San Diego, CA, USA: Elsevier; 2018. pp. 175–86.
Grundy SM, Stone NJ, Bailey AL, Beam C, Birtcher KK, Blumenthal RS, Braun LT, De Ferranti S, Faiella-Tommasino J, Forman DE, Goldberg R, AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA. /ASPC/NLA/PCNA guideline on the management of blood cholesterol: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation. 2019;139(25):e1082-143.].
Reed JL, Prince SA, Pipe AL, Attallah S, Adamo KB, Tulloch HE, Manuel D, Mullen KA, Fodor G, Reid RD. Influence of the workplace on physical activity and cardiometabolic health: Results of the multi-centre cross-sectional Champlain Nurses’ study. International journal of nursing studies. 2018; 1;81:49–60.
Download references
Acknowledgements
Not applicable.
Author information
Authors and affiliations.
Institute of Health Sciences, Medical College of Rzeszów University, Rejtana 16 C, 35-959, Rzeszów, Poland
Anna Bartosiewicz, Justyna Wyszyńska & Edyta Łuszczki
Institute of Physical Culture Sciences, Medical College of Rzeszów University, 35-959, Rzeszów, Poland
Piotr Matłosz
Department of Physiotherapy, Faculty of Health Sciences, Jagiellonian University Medical College, 31-007, Kraków, Poland
Łukasz Oleksy
Department of Orthopedics and Rehabilitation, Medical University of Warsaw, 04-749, Warsaw, Poland
Artur Stolarczyk
You can also search for this author in PubMed Google Scholar
Contributions
A.B. - development of the concept of research / scientific work, A.B., J.W., P.M, EŁ. - data compilation, A.B.– methodology, A.B. - analysis and interpretation of data, A.B. - writing an article, A.B., J.W. - substantive review article, Ł.O, A.S - Funding acquisition, A.B., J.W., E.Ł. - overseeing the final article. All authors reviewed the manuscript.
Corresponding author
Correspondence to Anna Bartosiewicz .
Ethics declarations
Ethics approval and consent to participate.
The study participants received verbal and written information about the objectives, risks, and benefits of the study. This study was approved by the Bioethics Committee of the University of Rzeszów (No. 2022/088) and was conducted in accordance with the ethical standards stated in the most recent version of the Declaration of Helsinki. Before the study was initiated, written consent was obtained from the nurses. The presented data do not contain any information that allows the respondents to be identified.
Consent for publication
Competing interests.
The authors declare no competing interests.
Additional information
Publisher’s note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary Material 1
Supplementary material 2, supplementary material 3, rights and permissions.
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ . The Creative Commons Public Domain Dedication waiver ( http://creativecommons.org/publicdomain/zero/1.0/ ) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
Reprints and permissions
About this article
Cite this article.
Bartosiewicz, A., Wyszyńska, J., Matłosz, P. et al. Prevalence of dyslipidaemia within Polish nurses. Cross-sectional study - single and multiple linear regression models and ROC analysis. BMC Public Health 24 , 1002 (2024). https://doi.org/10.1186/s12889-024-18542-6
Download citation
Received : 17 January 2024
Accepted : 07 April 2024
Published : 10 April 2024
DOI : https://doi.org/10.1186/s12889-024-18542-6
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Dislipidaemia
- Metabolic disorders
- Risk factors
BMC Public Health
ISSN: 1471-2458
- Submission enquiries: [email protected]
- General enquiries: [email protected]
IMAGES
VIDEO
COMMENTS
General health promoters. Health promotion by nurses is associated with common universal principles of nursing. The most common health promotion intervention used by nurses is health education (Robinson and Hill, 1998; Whitehead, 2001, 2007, 2011; Runciman et al., 2006; Witt and Puntel de Almeida, 2008; Parker et al., 2009).General health promoters are expected to have knowledge of health ...
Health Promotion: The Role of Nurses Essay. Nurses play a significant role in the promotion of health in the public sector. Each community has its own different culture, values, and beliefs. In this scenario, a nurse's work is to understand the principles and views of the community in which they are practicing their clinical work (Murdaugh et ...
As a nurse, you have a unique opportunity to assist your patients in leading a healthy lifestyle. This can be accomplished by promoting good habits, encouraging preventative care, and aiding in managing chronic conditions. This article will give you valuable insights into how you can emphasize health promotion and disease prevention among your ...
To further uncover the importance of the nursing role in health promotion, Whitehead explored the current position of nursing concerning its practice, associated concept, and policy . The questions raised included how much nurses know about HP and their views towards the subject of HP.
Role confusion is hampering the development of nurses' capacity for health promotion and prevention. Addressing this requires discussion to reach agreement among nurses, managers, co-workers, professional associations, academics and organisations about the nursing activities in this field. Forming a sound basis for this discussion is essential.
1. Define the scope of health promotion and disease prevention. 2. Discuss the nurse's role in promoting health and preventing illness. 3. Recognize the importance of patient education on health promotion and disease prevention. 4. Discuss elements of effective patient teaching and learning. 5.
Generally, nurses seem enthusiastic about health. promotion, and sure that they have a role to play. What is less certain is what this role is. The study seeks to clarify this by exploring policy, behaviour, and attitudes. Policy provides the framework for practice, and operates at a number of levels.
Phillips A (2019) Effective approaches to health promotion in nursing practice. Nursing Standard. doi: 10.7748/ns.2019.e11312. Accepted 19 November 2018. Published online: 04 March 2019. Keywords : behaviour change - health inequalities - health literacy - health promotion - lifestyles - patient education - patient empowerment - patients ...
Health promotion was clearly defined by O'Donnell (2002) as "the science and art of helping people change their lifestyle to move toward a state of optimal health.". This straightforward definition should resonate with nurs-es, who understand nursing as a helping profession that is both a science and an art.
A systematic review of existing research studies of health promotion roles by nurses finds that nurses play an important role in relation to health promotion in any setting like hospital, community, primary care and home care. Background: Promoting public health is applied by health care professionals including nurses. The focus of health promotion by nurses traditionally has been on disease ...
Aims and objectives: To provide a description of the state of nursing health promotion and prevention practice expressed in terms of activities classifiable under the Ottawa Charter and to reveal the misalignments between this portrayal and the ideal one proposed by the Ottawa Charter. Methods: A critical interpretive synthesis was conducted ...
Promotion One. First and foremost, nurses are the source of accurate information for their patients. In case of diabetes, this includes (but is not restricted to) the information about suitable lifestyle or proper insulin usage (Modic et al., 2014, p. 157). For example, the intensiveness of insulin therapy depends on the type of diabetes.
Health promotion can be defined using several definitions depending on the contextual application in nursing. In Richard et al (2008) article, health promotion is regarded as the measures put in place to ensure that individuals are cushioned against receiving injuries or various debilitating conditions. With regard to this, interventions and ...
Health Promotion. Nurses play an important role in promoting health within the patient, family, and community (Kemppainen, Tassavainen, & Turunen, 2012). The focus of patient care has been transferred from treating the illness to disease prevention (Mchugh, Robinson, & Chesters, 2010). The implementation of consultation, education, and follow ...
This study used concept analysis methodology to provide theoretical clarity for the concept of role models in health promoting behaviour for registered nurses and students. The framework included analysis of literature and qualitative data from six focus groups and one interview. Participants (n=39) included pre-registration students (adult ...
Nurses play an essential role in advancing the health of children by administering an immunization. "When functioning in a health promotion model" (Rankin 2005), each contact that nurse have with patients or their families is an opportunity to educate their patients or families. They advise parents on the excellent ways of taking care of their ...
Topics: Health, Health Promotion Words: 284 Pages: 1. A significant role in maintaining and forming the principles of a healthy lifestyle and motivation to preserve health is played by medical workers, particularly nurses. It is possible to form skills for maintaining health and the need to strengthen it at the preclinical stage.
Nurses play a multifaceted role in health promotion, encompassing education, cultural competence, and advocacy. Beyond clinical settings, nurses are instrumental in advocating for healthy behaviors and lifestyles. Initiatives such as smoking cessation and weight loss programs are examples of proactive health promotion.
In conclusion, with the emphasis of health promotion concerning the prevention of illness and disease, the role of the nurse is essential in raising awareness and providing education and advice to individuals to facilitate behaviour change. The complexities of health promotion indicate the extensive competences a nurse must possess to empower ...
Self-care, mindfulness, and client-centered therapy are major focuses in professional nursing. Nurses are challenged to be role models for their patients. Providing self-care demonstrates healthy lifestyle choices. Mindfulness also goes hand- in-hand with self-care because it helps people cope with stress.
This essay incorporates a health promotion scenario I was involved in during practice. The essay will critically analyze and discuss the actions and roles of a nurse in health promotion. It will also intend to explore some relevant definitions of health, health promotion, and the lay perception of health.
Health Promotion Essay. This written rationale will identify and explain the necessity for the promotion of public health and physical activity. It will demonstrate an understanding of the role, function and settings of public health and physical activity promotion by national, regional and local agencies. It will also analyse and evaluate the ...
The responsibility of a nurse in health promotion and education is considered as a major factor by numerous researchers and policy initiatives from the government to promote health, understanding that health promotion is essential. In the three journal articles selected for review from the GCU Library which incorporates the three levels of ...
Schools are important arenas for mental health promotion initiatives. School nurses have the opportunity and ability to support and promote students' mental health, but their role and practices have been perceived as somewhat unclear. Therefore, the aim of this study was to explore school nurses' mental health promotion practices.
Nurses are the largest medical profession in the world, accounting for almost 60% of all medical workers in the global health sector. They have great potential and play a pivotal role in providing care and treatment services [].However, due to stress, overwork, high patient demands and workplace hazards, the incidence of morbidity among healthcare workers is higher compared to the general ...