Obesity: Personal or Public Responsibility? Essay
Empirical arguments have provided the social, cultural, economic, and health justifications that obesity is more than just an issue concerning additional weight solely. Obesity is a personal health care responsibility. This vested responsibility implies that individuals should participate proactively and beyond a reasonable doubt in safeguarding healthy living. Obesity complications are associated with the choice of food eaten, and the shaped body takes as a result. The consumers should remain protected as well as educated on dietary habits as a way of enhancing their responsibility. The variables (environmental, economic, social, and health bottom-lines) affecting dietary choices as well as physical stature are largely manipulated in public. This makes it difficult for the majority to maintain an individual balance (based on these variables), particularly when prone to obesity complications. Based on a cost-benefit perspective and wide-scale impact assessment, a personalized approach will instill individual dietary discipline, while cushioning a shock from health risks involved. The public responsibility approach may be prone to finger-pointing or shifting blame, unnecessarily.
This means that due diligence should apply to avoid infringing the right to choice (and diversity) for the non-obese as well as to deny manufacturers the right to competitive bidding for a larger market share. Even if weight is gained due to eating fast foods at fast food retailers, an individual has the responsibility to control weight gaining (through fitness programs, for example) as well as understand their hereditary background which is linked to obesity problems. Before claiming a public agent, such as fast food retailer, to be responsible for the cause of obesity, hereditary or lack of fitness activities should be taken into account, and a preventive paradigm should substitute a damage control one. This negates the precautionary principle held by the due diligence concept. Public responsibility makes the food producer or manufacturer vulnerable to court cases and judicial decisions. The concept of demand-supply proves that personal responsibility referred to the customer demand for fast foods is the main power that forces the supplier to meet customer needs and requirements.
From a social and cultural perspective, legal action should focus on the individual right to choose as well as public education. Manufactured foods and fast food have wide market access across the world. Food manufacturers should legally be obliged to product labeling and explanation (duty to warn) to enhance consumer safety and awareness of the health risks involved. Obesity thrives against the backdrop of disparities in health care access and affordability. Moreover, there is a trend of a wealthy consumer lifestyle, which includes aggressive advertising that entices fast food addiction and market flooding of processed foods. These factors aggravate the proneness to obesity within a global society.
- Chicago (A-D)
- Chicago (N-B)
IvyPanda. (2021, February 13). Obesity: Personal or Public Responsibility? https://ivypanda.com/essays/obesity-personal-or-public-responsibility/
"Obesity: Personal or Public Responsibility?" IvyPanda , 13 Feb. 2021, ivypanda.com/essays/obesity-personal-or-public-responsibility/.
IvyPanda . (2021) 'Obesity: Personal or Public Responsibility'. 13 February.
IvyPanda . 2021. "Obesity: Personal or Public Responsibility?" February 13, 2021. https://ivypanda.com/essays/obesity-personal-or-public-responsibility/.
1. IvyPanda . "Obesity: Personal or Public Responsibility?" February 13, 2021. https://ivypanda.com/essays/obesity-personal-or-public-responsibility/.
Bibliography
IvyPanda . "Obesity: Personal or Public Responsibility?" February 13, 2021. https://ivypanda.com/essays/obesity-personal-or-public-responsibility/.
- Coffee Demand & Supply in the United Arab Emirates
- AT&T Inc.'s Products, Demand & Supply, and Market
- Effects of Obesity on Neuroendocrine, and Immune Cell Responses to Stress
- International Environmental Law: Precautionary Principle
- The role of the state in defending and/or infringing Native Indian Civil Rights in United States
- Childhood Obesity and Cold Virus
- Elevator Pitch for Kernel Keto Company
- Communicable Diseases and Precautionary Measures
- Equations for Predicting Resting Energy Expenditure
- Precautionary Principle in Environmental Situations
- Encultured Eating Course: Nine Weeks of Experience
- Humans Are Herbivores: Arguments For and Against
- Problem of Food Overconsumption
- Childhood Obesity and Food Culture in Schools
- "Quit Meat" Vegetarian Diet: Pros and Cons


Prevention, prevention, prevention.
Losing weight is hard to do.
In the U.S., only one in six adults who have dropped excess pounds actually keep off at least 10 percent of their original body weight. The reason: a mismatch between biology and environment. Our bodies are evolutionarily programmed to put on fat to ride out famine and preserve the excess by slowing metabolism and, more important, provoking hunger. People who have slimmed down and then regain their weight don’t lack willpower—their bodies are fighting them every inch of the way.
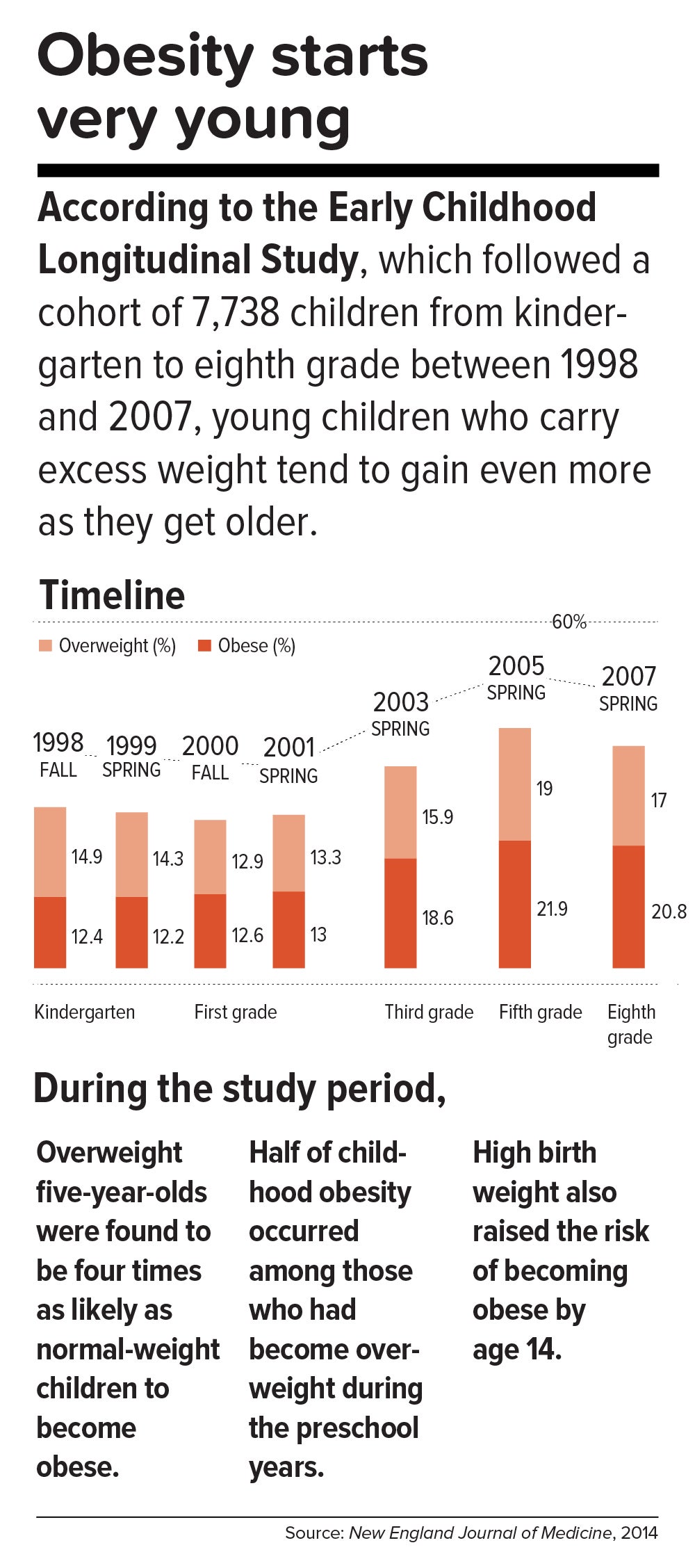
This inborn predisposition to hold on to added weight reverberates down the life course. Few children are born obese, but once they become heavy, they are usually destined to be heavy adolescents and heavy adults. According to a 2016 study in the New England Journal of Medicine , approximately 90 percent of children with severe obesity will become obese adults with a BMI of 35 or higher. Heavy young adults are generally heavy in middle and old age. Obesity also jumps across generations; having a mother who is obese is one of the strongest predictors of obesity in children.
All of which means that preventing child obesity is key to stopping the epidemic. By the time weight piles up in adulthood, it is usually too late. Luckily, preventing obesity in children is easier than in adults, partly because the excess calories they absorb are minimal and can be adjusted by small changes in diet—substituting water, for example, for sugary fruit juices or soda.
Still, the bulk of the obesity problem—literally—is in adults. According to Frank Hu, chair of the Harvard Chan Department of Nutrition, “Most people gain weight during young and middle adulthood. The weight-gain trajectory is less than 1 pound per year, but it creeps up steadily from age 18 to age 55. During this time, people gain fat mass, not muscle mass. When they reach age 55 or so, they begin to lose their existing muscle mass and gain even more fat mass. That’s when all the metabolic problems appear: insulin resistance, high cholesterol, high blood pressure.”
Adds Walter Willett, Frederick John Stare Professor of Epidemiology and Nutrition at Harvard Chan, “The first 5 pounds of weight gain at age 25—that’s the time to be taking action. Because someone is on a trajectory to end up being 30 pounds overweight by the time they’re age 50.”
The most realistic near-term public health goal, therefore, is not to reverse but rather to slow down the trend—and even this will require strong commitment from government at many levels. In May 2017, the Trump administration rolled back recently-enacted standards for school meals, delaying a rule to lower sodium and allowing waivers for regulations requiring cafeterias to serve foods rich in whole grains. If recent expansions in food entitlements and school meals are undermined, “It would be a ‘disaster,’ to use the president’s word,” says Marlene Schwartz, director of the Rudd Center for Obesity & Food Policy at the University of Connecticut. “The federal food programs are incredibly important, not just because of the food and money they provide families, but because supporting better nutrition in child care, schools, and the WIC [Women, Infants, and Children] program has created new social norms. We absolutely cannot undo the progress that we’ve made in helping this generation transition to a healthier diet.”
Get the science right.
It is impossible to prescribe solutions to obesity without reminding ourselves that nutrition scientists botched things decades ago and probably sent the epidemic into overdrive. Beginning in the 1970s, the U.S. government and major professional groups recommended for the first time that people eat a low-fat/high-carbohydrate diet. The advice was codified in 1977 with the first edition of The Dietary Goals for the United States , which aimed to cut diet-related conditions such as heart disease and diabetes. What ensued amounted to arguably the biggest public health experiment in U.S. history, and it backfired.
At the time, saturated fat and dietary cholesterol were believed to be the main factors responsible for cardiovascular disease—an oversimplified theory that ignored the fact that not all fats are created equal. Soon, the public health blitz against saturated fat became a war on all fat. In the American diet, fat calories plummeted and carb calories shot up.
“We can’t blame industry for this. It was a bandwagon effect in the scientific community, despite the lack of evidence—even with evidence to the contrary,” says Willett. “Farmers have known for thousands of years that if you put animals in a pen, don’t let them run around, and load them up with grains, they get fat. That’s basically what has been happening to people: We created the great American feedlot. And we added in sugar, coloring, and seductive promotion for low-fat junk food.”
Scientists now know that whole fruits and vegetables (other than potatoes), whole grains, high-quality proteins (such as from fish, chicken, beans, and nuts), and healthy plant oils (such as olive, peanut, or canola oil) are the foundations of a healthy diet.
But there is also a lot scientists don’t yet know. One unanswered question is why some people with obesity are spared the medical complications of excess weight. Another concerns the major mechanisms by which obesity ushers in disease. Although surplus body weight can itself directly cause problems—such as arthritis due to added load on joints, or breast cancer caused by hormones secreted by fat cells—in general, obesity triggers myriad biological processes. Many of the resulting conditions—such as atherosclerosis, diabetes, and even Alzheimer’s disease—are mediated by inflammation, in which the body’s immune response becomes damagingly self-perpetuating. In this sense, today’s food system is as inflammagenic as it is obesigenic.
Scientists also need to ferret out the nuanced effects of particular foods. For example, do fermented products—such as yogurt, tempeh, or sauerkraut—have beneficial properties? Some studies have found that yogurt protects against weight gain and diabetes, and suggest that healthy live bacteria (known as probiotics) may play a role. Other reports point to fruits being more protective than vegetables in weight control and diabetes prevention, although the types of fruits and vegetables make a difference.
A 2017 article in the American Journal of Clinical Nutrition showed that substituting whole grains for refined grains led to a loss of nearly 100 calories a day—by speeding up metabolism, cutting the number of calories that the body hangs on to, and, more surprisingly, by changing the digestibility of other foods on the plate. That extra energy lost daily—by substituting, say, brown rice for white rice or barley for pita bread—was equivalent to a brisk 30-minute walk. One hundred calories a day, sustained over years, and multiplied by the population is one mathematical equivalent of the obesity epidemic.
A companion study found that adults who ate a whole-grain-rich diet developed healthier gut bacteria and improved immune responses. That particular foods alter the gut microbiome—the dense and vital community of bacteria and other microorganisms that work symbiotically with the body’s own digestive system—is another critical insight. The microbiome helps determine weight by controlling how our bodies extract calories and store fat in the liver, and the microbiomes of obese individuals are startlingly efficient at harvesting calories from food. [To learn more about Harvard Chan research on the gut microbiome, read “ Bugs in the System .”] The hormonal effects of sleep deprivation and stress—two epidemics concurrent and intertwined with the obesity trend—are other promising avenues of research.
And then there are the mystery factors. One recent hypothesis is that an agent known as adenovirus 36 partly accounts for our collective heft. A 2010 article in The Royal Society described a study in which researchers examined samples of more than 20,000 animals from eight species living with or around humans in industrialized nations, a menagerie that included macaques, chimpanzees, vervets, marmosets, lab mice and rats, feral rats, and domestic dogs and cats. Like their Homo sapiens counterparts, all of the study populations had gained weight over the past several decades—wild, domestic, and lab animals alike. The chance that this is a coincidence is, according to the scientists’ estimate, 1 in 10 million. The stumped authors surmise that viruses, gene expression changes, or “as-of-yet unidentified and/or poorly understood factors” are to blame.
Master the art of persuasion.
A 2015 paper in the American Journal of Public Health revealed the philosophical chasm that hampers America’s progress on obesity prevention. It found that 72 to 98 percent of obesity-related media reports emphasize personal responsibility for weight, compared with 40 percent of scientific papers.
A recent study by Drexel University researchers also quantified the political polarization around public health measures. From 1998 through 2013, Democrats voted in line with recommendations from the American Public Health Association 88.3 percent of the time, on average, while Republicans voted for the proposals just 21.3 percent of the time.
Clearly, we can’t count on bipartisan goodwill to stem the obesity crisis. But we can ask what kinds of messages appeal to politically divergent audiences. A stealth strategy may be to avoid even uttering the word “obesity.” On January 1 of this year, Philadelphia’s 1.5-cents-per-ounce excise tax on sugar-sweetened and diet beverages took effect. When Philadelphia Mayor Jim Kenney lobbied voters to approve the tax, his bid centered not on improving health—the unsuccessful pitch of his predecessor—but on raising $91 million annually for prekindergarten programs.
“That’s something lots of people care about and can get behind—it’s a feel-good policy, and it makes sense,” says psychologist Christina Roberto, assistant professor of medical ethics and health policy at the University of Pennsylvania, and a former assistant professor of social and behavioral sciences and nutrition at Harvard Chan. The provision for taxing diet beverages was also shrewd, she adds, because it spread the tax’s pain; since wealthier people are more likely than less-affluent individuals to buy diet drinks, the tax could not be slapped with the label “regressive.”
But Roberto sees a larger lesson in the Philadelphia story. Public health messaging that appeals to values that transcend the individual is less fraught, less stigmatizing, and perhaps more effective. As she puts it, “It’s very different to hear the message, ‘Eat less red meat, help the planet’ versus ‘Eat less red meat, help yourself avoid saturated fat and cardiovascular disease.’”
Supermarket makeovers
Supermarket aisles are other places where public health can shuffle a deck stacked against healthy consumer choices.
With slim profit margins and 50,000-plus products on their shelves, grocery stores depend heavily on food manufacturers’ promotional incentives to make their bottom lines. “Manufacturers pay slotting fees to get their products on the shelf, and they pay promotion allowances: We’ll give you this much off a carton of Coke if you put it on sale for a certain price or if you put it on an end-of-aisle display,” says José Alvarez, former president and chief executive officer of Stop & Shop/Giant-Landover, now senior lecturer of business administration at Harvard Business School. Such promotional payments, Alvarez adds, often exceed retailers’ net profits.
Healthy new products—like flash-frozen dinners prepared with heaps of vegetables and whole grains, and relatively little salt—can’t compete for prized shelf space against boxed mac and cheese or cloying breakfast cereals. One solution, says Alvarez, is for established consumer packaged goods companies to buy out what he calls the “hippie in the basement” firms that have whipped up more nutritious items. The behemoths could apply their production, marketing, and distribution prowess to the new offerings—and indeed, this has started to happen over the last five years.
Another approach is to make nutritious foods more convenient to eat. “We have all of these cooking shows and upscale food magazines, but most people don’t have the time or inclination—or the skills, quite frankly—to cook,” says Alvarez. “Instead, we should focus on creating high-quality, healthy, affordable prepared foods.”
An additional model is suggested by Jeff Dunn, a 20-year veteran of the soft drink industry and former president of Coca-Cola North America, who went on to become an advocate for fresh, healthy food. Dunn served as president and chief executive officer of Bolthouse Farms from 2008 to 2015, where he dramatically increased sales of baby carrots by using marketing techniques common in the junk food business. “We operated on the principles of the three 3 A’s: accessibility, availability, and affordability,” says Dunn. “That, by the way, is Coke’s more-than-70-year-old formula for success.”
Show them the money.
Obesity kills budgets. According to the Campaign to End Obesity, a collaboration of leaders from industry, academia, public health, and policymakers, annual U.S. health costs related to obesity approach $200 billion. In 2010, the nonpartisan Congressional Budget Office reported that nearly 20 percent of the rise in health care spending from 1987 to 2007 was linked to obesity. And the U.S. Centers for Disease Control and Prevention (CDC) found that full-time workers in the U.S. who are overweight or obese and have other chronic health conditions miss an estimated 450 million more days of work each year than do healthy employees—upward of $153 billion in lost productivity annually.
But making the money case for obesity prevention isn’t straightforward. For interventions targeting children and youth, only a small fraction of savings is captured in the first decade, since most serious health complications don’t emerge for many years. Long-term obesity prevention, in other words, doesn’t fit into political timetables for elected officials.
Yet lawmakers are keen to know how “best for the money” obesity-prevention programs can help them in the short run. Over the past two years, Harvard Chan’s Steve Gortmaker and his colleagues have been working with state health departments in Alaska, Mississippi, New Hampshire, Oklahoma, Washington, and West Virginia and with the city of Philadelphia and other locales, building cost-effectiveness models using local data for a wide variety of interventions—from improved early child care to healthy school environments to communitywide campaigns. “We collaborate with health departments and community stakeholders, provide them with the evidence base, help assess how much different options cost, model the results over a decade, and they pick what they want to work on. One constant that we’ve seen—and these are very different political environments—is a strong interest in cost-effectiveness,” he says.
In a 2015 study in Health Affairs , Gortmaker and colleagues outlined three interventions that would more than pay for themselves: an excise tax on sugar-sweetened beverages implemented at the state level; elimination of the tax subsidy for advertising unhealthy food to children; and strong nutrition standards for food and drinks sold in schools outside of school meals. Implemented nationally, these interventions would prevent 576,000, 129,100, and 345,000 cases of childhood obesity, respectively, by 2025. The projected net savings to society in obesity-related health care costs for each dollar invested: $31, $33, and $4.60, respectively.
Gortmaker is one of the leaders of a collaborative modeling effort known as CHOICES—for Childhood Obesity Intervention Cost-Effectiveness Study—an acronym that seems a pointed rebuttal to the reflexive conservative argument that government regulation tramples individual choice. Having grown up not far from Des Plaines, Illinois, site of the first McDonald’s franchise in the country, he emphasizes to policymakers that at this late date, America cannot treat its way out of obesity, given current medical know-how. Only a thoroughgoing investment in prevention will turn the tide. “Clinical interventions produce too small an effect, with too small a population, and at high cost,” Gortmaker says. “The good news is that there are many cost-effective options to choose from.”
While Gortmaker underscores the importance of improving both food choices and options for physical activity, he has shown that upgrading the food environment offers much more benefit for the buck. This is in line with the gathering scientific consensus that what we eat plays a greater role in obesity than does sedentary lifestyle (although exercise protects against many of the metabolic consequences of excess weight). “The easiest way to explain it,” Gortmaker says, “is to talk about a sugary beverage—140 calories. You could quickly change a kid’s risk of excess energy balance by 140 calories a day just by switching from a sugary drink a day to water or sparkling water. But for a 10-year-old boy to burn an extra 140 calories, he’d have to replace an hour-and-a-half of sitting with an hour-and-a-half of walking.”
Small tweaks in adults’ diets can likewise make a big difference in short order. “With adults, health care costs rise rapidly with excess weight gain,” Gortmaker says. “If you can slow the onset of obesity, you slow the onset of diabetes, and potentially not only save health care costs but also boost people’s productivity in the workforce.”
One of Gortmaker’s most intriguing calculations spins off of the food industry’s estimated $633 million spent on television marketing aimed at kids. Currently, federal tax treatment of advertising as an ordinary business expense means that the government, in effect, subsidizes hawking of junk food to children. Gortmaker modeled a national intervention that would eliminate this subsidy of TV ads for nutritionally empty foods and beverages aimed at 2- to 19-year-olds. Drawing on well-delineated relationships between exposure to these advertisements and subsequent weight gain, he found that the intervention would save $260 million in downstream health care costs. Although the effect would probably be small at the individual level, it would be significant at the population level.

Level the playing field through taxes and regulation.
When public health took on cigarette smoking, starting in the 1960s, it did so with robust policies banning television ads and other marketing, raising taxes to increase prices, making public places smoke-free, and offering people treatment such as the nicotine patch. In 1965, the smoking rate for U.S. adults was 42.2 percent; today, it is 16.8 percent.
Similarly, America reduced the rate of deaths caused by motor vehicle accidents—a 90 percent decrease over the 20th century, according to the CDC—with mandatory seat belt laws, safer car designs, stop signs, speed limits, rumble strips, and the stigmatization of drunk driving.
Change the product. Change the environment. Change the culture. That is also the policy recipe for stopping obesity.
Laws that make healthy behaviors easier are often followed by positive changes in those behaviors. And people who are trying to adopt healthy behaviors tend to support policies that make their personal aspirations achievable, which in turn nudges lawmakers to back the proposals.
One debate today revolves around whether recipients of federal Supplemental Nutrition Assistance Program (SNAP) benefits (formerly known as food stamps) should be restricted from buying sodas or junk food. The largest component of the USDA budget, SNAP feeds one in seven Americans. A USDA report, issued last November, found that the number-one purchase by SNAP households was sweetened beverages, a category that included soft drinks, fruit juices, energy drinks, and sweetened teas, accounting for nearly 10 percent of SNAP money spent on food. Is the USDA therefore underwriting the soda industry and planting the seeds for chronic disease that the government will pay to treat years down the line?
Eric Rimm, a professor in the Departments of Epidemiology and Nutrition at the Harvard Chan School, frames the issue differently. In a 2017 study in the American Journal of Preventive Medicine , he and his colleagues asked SNAP participants whether they would prefer the standard benefits package or a “SNAP-plus” that prohibited the purchase of sugary beverages but offered 50 percent more money for buying fruits and vegetables. Sixty-eight percent of the participants chose the healthy SNAP-plus option.
“A lot of work around SNAP policy is done by academics and politicians, without reaching out to the beneficiaries,” says Rimm. “We haven’t asked participants, ‘What’s your say in this? How can we make this program better for you?’” To be sure, SNAP is riddled with nutritional contradictions. Under current rules, for example, participants can use benefits to buy a 12-pack of Pepsi or a Snickers bar or a giant bag of Lay’s potato chips but not real food that happens to be heated, such as a package of rotisserie chicken. “This is the most vulnerable population in the country,” says Rimm. “We’re not listening well enough to our constituency.”
Other innovative fiscal levers to alter behavior could also drive down obesity. In 2014, a trio of strong voices on food industry practices—Dariush Mozaffarian, DrPH ’06, dean of Tufts University’s Friedman School of Nutrition Science and Policy and former associate professor of epidemiology at the Harvard Chan School; Kenneth Rogoff, professor of economics at Harvard; and David Ludwig, professor in the Department of Nutrition at Harvard Chan and a physician at Boston Children’s Hospital—broached the idea of a “meaningful” tax on nearly all packaged retail foods and many chain restaurants, with the proceeds used to pay for minimally processed foods and healthier meals for school kids. In essence, the tax externalizes the social costs of harmful individual behavior.
“We made a straightforward proposal to tax all processed foods and then use the income to subsidize whole foods in a short-term, revenue-neutral way,” explains Ludwig. “The power of this idea is that, since there is so much processed food consumption, even a modest tax—in the 10 to 15 percent range—is not going to greatly inflate the cost of these foods. Their price would increase moderately, but the proceeds would not disappear into government coffers. Instead, the revenue would make healthy foods affordable for virtually the entire population, and the benefits would be immediately evident. Yes, people will pay moderately more for their Coke or for their cinnamon bear claw but a lot less for nourishing, whole foods.”
Another suggestion comes from Sandro Galea, dean of the Boston University School of Public Health, and Abdulrahman M. El-Sayed, a public health physician and epidemiologist. In a 2015 issue of the American Journal of Public Health , they called for “calorie offsets,” similar to the carbon offsets used to mitigate environmental harm caused by the gas and oil industries. A “calorie offset” scheme could hand the food and beverage industries a chance at redemption by inviting them to invest in such undertakings as city farms, cooking classes for parents, healthy school cafeterias, and urban green spaces.
These ambitious proposals face almost impossibly high hurdles. Political battle lines typically pit public health against corporations, with Big Food casting doubt on solid nutrition science, deeming government regulation a threat to free choice, and making self-policing pledges that it has never kept. On the website for the Americans for Food and Beverage Choice, a group spearheaded by the American Beverage Association, is the admonition: “[W]hether it’s at a restaurant or in a grocery store, it’s never the government’s job to decide what you choose to eat and drink.”
Yet surprisingly, many public health professionals are convinced that the only way to stop obesity is to make common cause with the food industry. “This isn’t like tobacco, where it’s a fight to the death. We need the food industry to make healthier food and to make a profit,” says Mozaffarian. “The food industry is much more diverse and heterogeneous than tobacco or even cars. As long as we can help them—through carrots and sticks, tax incentives and disincentives—to move towards healthier products, then they are part of the solution. But we have to be vigilant, because they use a lot of the same tactics that tobacco did.”
Sow what we want to reap.
Americans overeat what our farmers overproduce.
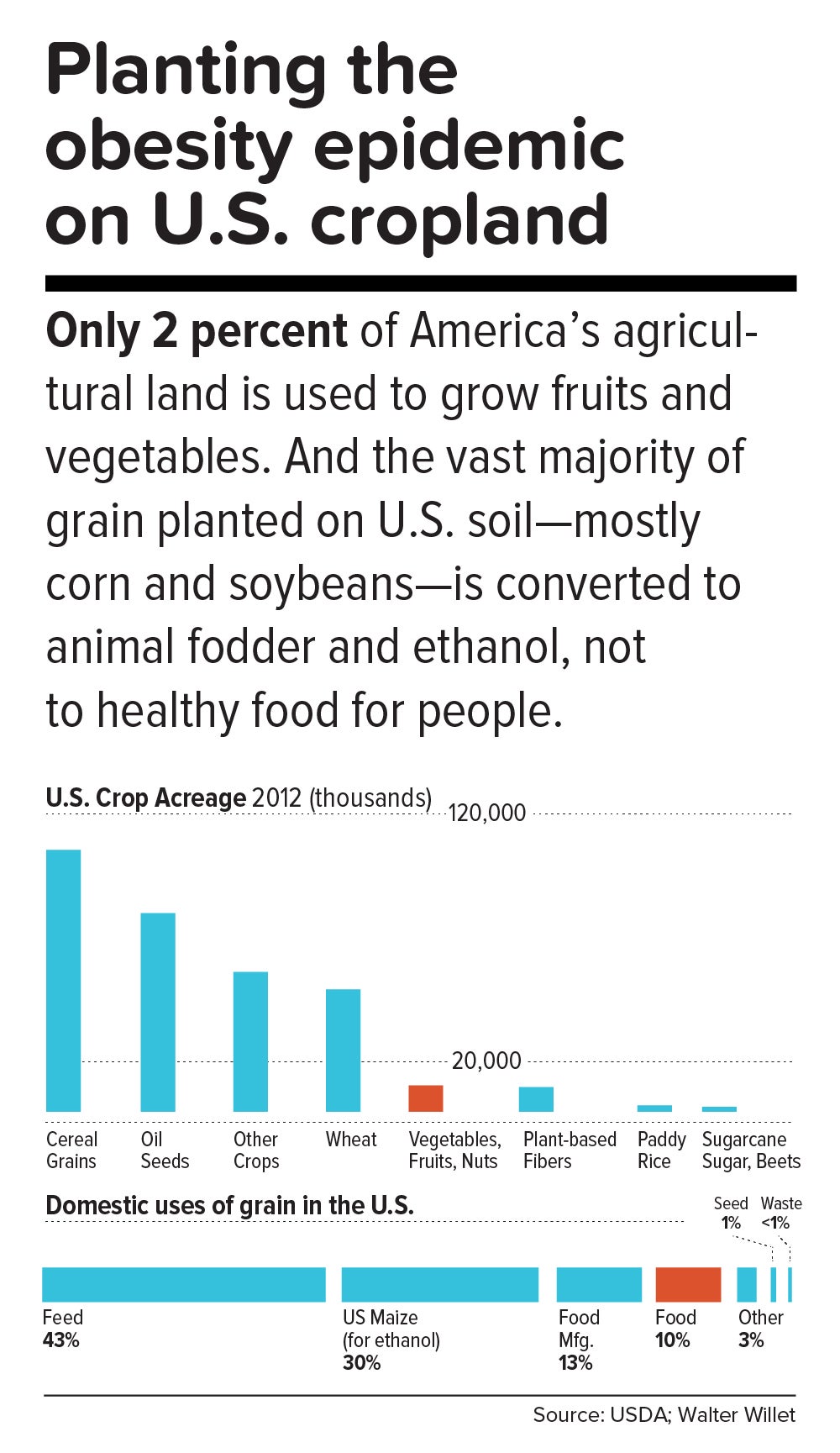
“The U.S. food system is egregiously terrible for human and planetary health,” says Walter Willett. It’s so terrible, Willett made a pie chart of American grain production consumed domestically. It shows that most of the country’s agricultural land goes to the two giant commodity crops: corn and soy. Most of those crops, in turn, go to animal fodder and ethanol, and are also heavily used in processed snack foods. Today, only about 10 percent of grain grown in the U.S. for domestic use is eaten directly by human beings. According to a 2013 report from the Union of Concerned Scientists, only 2 percent of U.S. farmland is used to grow fruits and vegetables, while 59 percent is devoted to commodity crops.
Historically, those skewed proportions made sense. Federal food policies, drafted with the goal of alleviating hunger, preferentially subsidize corn and soy production. And whereas corn or soybeans could be shipped for days on a train, fruits and vegetables had to be grown closer to cities by truck farmers so the produce wouldn’t spoil. But those long-ago constraints don’t explain today’s upside-down agricultural priorities.
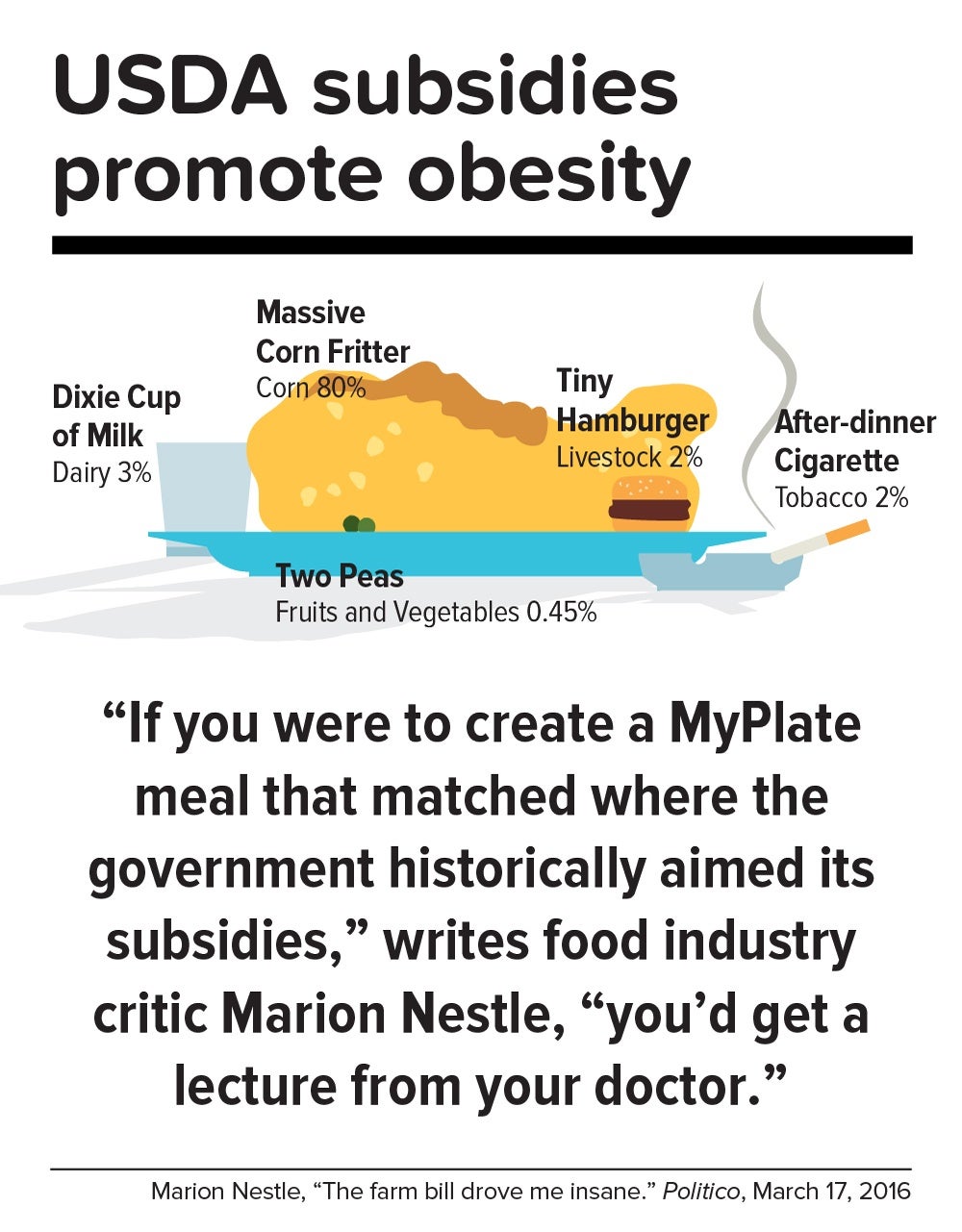
In a now-classic 2016 Politico article titled “The farm bill drove me insane,” Marion Nestle illustrated the irrational gap between what the government recommends we eat and what it subsidizes: “If you were to create a MyPlate meal that matched where the government historically aimed its subsidies, you’d get a lecture from your doctor. More than three-quarters of your plate would be taken up by a massive corn fritter (80 percent of benefits go to corn, grains and soy oil). You’d have a Dixie cup of milk (dairy gets 3 percent), a hamburger the size of a half dollar (livestock: 2 percent), two peas (fruits and vegetables: 0.45 percent) and an after-dinner cigarette (tobacco: 2 percent). Oh, and a really big linen napkin (cotton: 13 percent) to dab your lips.”
In this sense, the USDA marginalizes human health. Many of the foods that nutritionists agree are best for us—notably, fruits, vegetables, and tree nuts—fall under the bureaucratic rubric “specialty crops,” a category that also includes “dried fruits, horticulture, and nursery crops (including floriculture).” Farm bills, which get passed every five years or so, fortify the status quo. The 2014 Farm Bill, for example, provided $73 million for the Specialty Crop Block Grant Program in 2017, out of a total of about $25 billion for the USDA’s discretionary budget. (The next Farm Bill, now under debate, will be coming out in 2018.)
By contrast, a truly anti-obesigenic agricultural system would stimulate USDA support for crop diversity—through technical assistance, research, agricultural training programs, and financial aid for farmers who are newly planting or transitioning their land into produce. It would also enable farmers, most of whom survive on razor-thin profit margins, to make a decent living.
In the early 1970s, Finland’s death rate from coronary heart disease was the highest in the world, and in the eastern region of North Karelia—a pristine, sparsely populated frontier landscape of forest and lakes—the rate was 40 percent worse than the national average. Every family saw physically active men, loggers and farmers who were strong and lean, dying in their prime.
Thus was born the North Karelia Project, which became a model worldwide for saving lives by transforming lifestyles. The project was launched in 1972 and officially ended 25 years later. While its initial goal was to reduce smoking and saturated fat in the diet, it later resolved to increase fruit and vegetable consumption.
The North Karelia Project fulfilled all of these ambitions. When it started, for example, 86 percent of men and 82 percent of women smeared butter on their bread; by the early 2000s, only 10 percent of men and 4 percent of women so indulged. Use of vegetable oil for cooking jumped from virtually zero in 1970 to 50 percent in 2009. Fruit and vegetables, once rare visitors to the dinner plate, became regulars. Over the project’s official quarter-century existence, coronary heart disease deaths in working-age North Karelian men fell 82 percent, and life expectancy rose seven years.
The secret of North Karelia’s success was an all-out philosophy. Team members spent innumerable hours meeting with residents and assuring them that they had the power to improve their own health. The volunteers enlisted the assistance of an influential women’s group, farmers’ unions, homemakers’ organizations, hunting clubs, and church congregations. They redesigned food labels and upgraded health services. Towns competed in cholesterol-cutting contests. The national government passed sweeping legislation (including a total ban on tobacco advertising). Dairy subsidies were thrown out. Farmers were given strong incentives to produce low-fat milk, or to get paid for meat and dairy products based not on high-fat but on high-protein content. And the newly established East Finland Berry and Vegetable Project helped locals switch from dairy farming—which had made up more than two-thirds of agriculture in the region—to cultivation of cold-hardy currants, gooseberries, and strawberries, as well as rapeseed for heart-healthy canola oil.
“A mass epidemic calls for mass action,” says the project’s director, Pekka Puska, “and the changing of lifestyles can only succeed through community action. In this case, the people pulled the government—the government didn’t pull the people.”
Could the United States in 2017 learn from North Karelia’s 1970s grand experiment?
“Americans didn’t become an obese nation overnight. It took a long time—several decades, the same timeline as in individuals,” notes Frank Hu. “What were we doing over the past 20 years or 30 years, before we crossed this threshold? We haven’t asked these questions. We haven’t done this kind of soul-searching, as individuals or society as a whole.”
Today, Americans may finally be willing to take a hard look at how food figures in their lives. In a July 2015 Gallup phone poll of Americans 18 and older, 61 percent said they actively try to avoid regular soda (the figure was 41 percent in 2002); 50 percent try to avoid sugar; and 93 percent try to eat vegetables (but only 57.7 percent in 2013 reported they ate five or more servings of fruits and vegetables at least four days of the previous week).
Individual resolve, of course, counts for little in problems as big as the obesity epidemic. Most successes in public health bank on collective action to support personal responsibility while fighting discrimination against an epidemic’s victims. [To learn more about the perils of stigma against people with obesity, read “ The Scarlet F .”]
Yet many of public health’s legendary successes also took what seems like an agonizingly long time to work. Do we have that luxury?
“Right now, healthy eating in America is like swimming upstream. If you are a strong swimmer and in good shape, you can swim for a little while, but eventually you’re going to get tired and start floating back down,” says Margo Wootan, SD ’93, director of nutrition policy for the Center for Science in the Public Interest. “If you’re distracted for a second—your kid tugs on your pant leg, you had a bad day, you’re tired, you’re worried about paying your bills—the default options push you toward eating too much of the wrong kinds of food.”
But Wootan has not lowered her sights. “What we need is mobilization,” she says. “Mobilize the public to address nutrition and obesity as societal problems—recognizing that each of us makes individual choices throughout the day, but that right now the environment is stacked against us. If we don’t change that, stopping obesity will be impossible.”
The passing of power to younger generations may aid the cause. Millennials are more inclined to view food not merely as nutrition but also as narrative—a trend that leaves Duke University’s Kelly Brownell optimistic. “Younger people have been raised to care about the story of their food. Their interest is in where it came from, who grew it, whether it contributes to sustainable agriculture, its carbon footprint, and other factors. The previous generation paid attention to narrower issues, such as hunger or obesity. The Millennials are attuned to the concept of food systems.”
We are at a public health inflection point. Forty years from now, when we gaze at the high-resolution digital color photos from our own era, what will we think? Will we realize that we failed to address the obesity epidemic, or will we know that we acted wisely?
The question brings us back to the 1970s, and to Pekka Puska, the physician who directed the North Karelia Project during its quarter-century existence. Puska, now 71, was all of 27 and burning with big ideas when he signed up to lead the audacious effort. He knows the promise and the perils of idealism. “Changing the world may have been utopic,” he says, “but changing public health was possible.”
News from the School

From public servant to public health student

Exploring the intersection of health, mindfulness, and climate change

Conference aims to help experts foster health equity

Building solidarity to face global injustice
The Role of Personal Responsibility in the Obesity Epidemic
How the power of the “eat more” food environment can overcome our conscious controls.
Below is an approximation of this video’s audio content. To see any graphs, charts, graphics, images, and quotes to which Dr. Greger may be referring, watch the above video.
Food and beverage companies frame body weight as a matter of personal choice. Even when we’re not distracted, the power of the “eat more” food environment may sometimes overcome our conscious controls over eating. One look around the room at a dietician convention can tell you that even nutrition professionals are vulnerable to the aggressively marketed ubiquity of tasty, cheap, convenient calories. This suggests there are aspects of our eating behaviors that defy personal insight by flying below the radar of conscious awareness. Appetite physiologists call the result of these subconscious actions “passive overconsumption.”
Remember that brain scan study where the thought of a milkshake lit up the same reward pathways in the brain as substance abuse? That was triggered just by a picture of a milkshake. Dopamine gets released, cravings get activated, and we’re motivated to eat. Intellectually, we know it’s just an image, but our lizard brain just sees survival. It’s just a reflexive response over which we have little control––which is why marketers ensure there are pictures of milkshakes and their equivalents everywhere.
Maintaining a balance between calories in and calories out feels like a series of voluntary acts under conscious control, but it may be more akin to bodily functions such as blinking, breathing, coughing, swallowing, or sleeping. You can try to will yourself power over any of these, but by and large, they just happen automatically, driven by ancient scripts.
Not only are food ads ubiquitous; so is the food. The types of establishments selling food products expanded dramatically in the 1970s and 1980s. Now there’s candy and snacks at the checkout counters of gas stations, drug stores, bookstores, and places that used to just sell clothes, hardware, home furnishings, or building supplies. The largest food retailer in the United States is Walmart. There’s that jolt of dopamine, and the artificially-stimulated feelings of hunger around every turn. Every day we run the gauntlet.
And it’s become socially acceptable to eat anywhere—in your car, on the street, or packed in a crowded bus. We’ve become a snacking society. Vending machines are everywhere. Daily eating episodes seem to have gone up by about a quarter since the late 1970s––increasing from about four to five occasions a day, potentially accounting for twice the calorie increase attributed to increasing portion sizes. Snacks and beverages alone could account for the bulk of the calorie surplus implicated in the obesity epidemic.
And think of the children. Here we are trying to do the best for our kids, role-modeling healthy habits, feeding them healthy foods, but then they venture out into a veritable tornado of junky food and manipulative messages. This commentary in the New England Journal of Medicine asked why should our efforts to protect our children from life-threatening illness be undermined by massive marketing campaigns from the manufacturers of junk food. Pediatricians are now encouraged to have the “french fry discussion” with parents at the 12-month well-child visit and not wait all the way until year two. And even that may be too late. Two-thirds of infants are being fed junk food by their first birthday.
Dr. David Katz may have said it best in the Harvard Health Policy Review : “Those who contend that parental or personal responsibility should carry the day despite these environmental temptations might consider the implications of generalizing the principle. Perhaps children should be encouraged, but not required, to attend school, and tempted each morning by alternatives, such as buses to the circus, zoo, or beach.”
Please consider volunteering to help out on the site.
- Nestle M. Utopian dream: a new farm bill. Dissent. 2012;59(2):15-9.
- Cohen DA. Neurophysiological pathways to obesity: below awareness and beyond individual control. Diabetes. 2008;57(7):1768-73.
- Swinburn BA, Sacks G, Hall KD, et al. The global obesity pandemic: shaped by global drivers and local environments. Lancet. 2011;378(9793):804-14.
- Gearhardt AN, Yokum S, Orr PT, Stice E, Corbin WR, Brownell KD. Neural correlates of food addiction. Arch Gen Psychiatry. 2011;68(8):808-16.
- Zimmerman FJ. Using marketing muscle to sell fat: the rise of obesity in the modern economy. Annu Rev Public Health. 2011;32:285-306.
- Taillie LS, Ng SW, Popkin BM. Global growth of “big box” stores and the potential impact on human health and nutrition. Nutr Rev. 2016;74(2):83-97.
- Nestle M. Counting the cost of calories. Interview by Ben Jones. Bull World Health Organ. 2012;90(8):566-7.
- Duffey KJ, Popkin BM. Energy density, portion size, and eating occasions: contributions to increased energy intake in the United States, 1977–2006. PLoS Med. 2011;8(6):e1001050.
- Ludwig DS. Childhood obesity—the shape of things to come. N Engl J Med. 2007;357(23):2325-7.
- Bonnet J, George A, Evans P, Silberberg M, Dolinsky D. Rethinking obesity counseling: having the French Fry Discussion. J Obes. 2014;2014:525021.
- Grummer-Strawn LM, Scanlon KS, Fein SB. Infant feeding and feeding transitions during the first year of life. Pediatrics. 2008;122 Suppl 2:S36-42.
- Katz D. Obesity . . . be dammed!: what it will take to turn the tide. Harvard Health Policy Rev. 2006;7(2):135-51.
Acknowledgements
Video production by Glass Entertainment
Motion graphics by Avocado Video
- Dr. David Katz
- processed foods
- weight gain
- weight loss
View Transcript
Sources cited, republishing "the role of personal responsibility in the obesity epidemic".
You may republish this material online or in print under our Creative Commons licence . You must attribute the article to NutritionFacts.org with a link back to our website in your republication.
If any changes are made to the original text or video, you must indicate, reasonably, what has changed about the article or video.
You may not use our material for commercial purposes.
You may not apply legal terms or technological measures that restrict others from doing anything permitted here.
If you have any questions, please Contact Us
Creative Commons Attribution-NonCommercial 4.0 International (CC BY-NC 4.0)
Doctor's note.
It can be helpful, perhaps, to take a step back and think of what’s at stake here. We’re not just talking about being manipulated into buying a different brand of toothpaste. The obesity pandemic has resulted in millions of deaths and untold suffering. And if you’re not mad yet, brace yourself for my next video, The Role of Corporate Influence in the Obesity Epidemic .
This is the ninth in this 11-part series. If you missed any, see:
- The Role of Diet vs. Exercise in the Obesity Epidemic
- The Role of Genes in the Obesity Epidemic
- The Thrifty Gene Theory: Survival of the Fattest
- Cut the Calorie-Rich-And-Processed Foods
- The Role of Processed Foods in the Obesity Epidemic
- The Role of Taxpayer Subsidies in the Obesity Epidemic
- The Role of Marketing in the Obesity Epidemic
The Role of Food Advertisements in the Obesity Epidemic
If you haven’t yet, you can subscribe to my videos for free by clicking here . Read our important information about translations here .
Subscribe to our free newsletter and receive our Daily Dozen Meal Planning Guide .
Flashback Friday: Coffee and Mortality
Subscribe to nutritionfacts.org videos.
By subscribing, you will automatically receive the latest videos emailed to you or downloaded to your computer or portable device. Select the subscription method below that best fits your lifestyle.

Or subscribe with your favorite app by using the address below:
iOS (iPhone, iPad, and iPod)
To subscribe, select the "Subscribe on iTunes" button above.
To subscribe, select the "Subscribe via E-Mail" button above.
Mac and Windows
Android and amazon fire.
To subscribe, select the "Subscribe on Android" button above.
Using Your Favorite Application
Copy the address found in the box above and paste into your favorite podcast application or news reader.
Bookmarking NutritionFacts.org
To bookmark this site, press the Ctrl + D keys on your Windows keyboard, or Command + D for Mac.
Pin It on Pinterest
- Search Menu
- Browse content in Arts and Humanities
- Browse content in Archaeology
- Anglo-Saxon and Medieval Archaeology
- Archaeological Methodology and Techniques
- Archaeology by Region
- Archaeology of Religion
- Archaeology of Trade and Exchange
- Biblical Archaeology
- Contemporary and Public Archaeology
- Environmental Archaeology
- Historical Archaeology
- History and Theory of Archaeology
- Industrial Archaeology
- Landscape Archaeology
- Mortuary Archaeology
- Prehistoric Archaeology
- Underwater Archaeology
- Urban Archaeology
- Zooarchaeology
- Browse content in Architecture
- Architectural Structure and Design
- History of Architecture
- Residential and Domestic Buildings
- Theory of Architecture
- Browse content in Art
- Art Subjects and Themes
- History of Art
- Industrial and Commercial Art
- Theory of Art
- Biographical Studies
- Byzantine Studies
- Browse content in Classical Studies
- Classical History
- Classical Philosophy
- Classical Mythology
- Classical Literature
- Classical Reception
- Classical Art and Architecture
- Classical Oratory and Rhetoric
- Greek and Roman Epigraphy
- Greek and Roman Law
- Greek and Roman Papyrology
- Greek and Roman Archaeology
- Late Antiquity
- Religion in the Ancient World
- Digital Humanities
- Browse content in History
- Colonialism and Imperialism
- Diplomatic History
- Environmental History
- Genealogy, Heraldry, Names, and Honours
- Genocide and Ethnic Cleansing
- Historical Geography
- History by Period
- History of Emotions
- History of Agriculture
- History of Education
- History of Gender and Sexuality
- Industrial History
- Intellectual History
- International History
- Labour History
- Legal and Constitutional History
- Local and Family History
- Maritime History
- Military History
- National Liberation and Post-Colonialism
- Oral History
- Political History
- Public History
- Regional and National History
- Revolutions and Rebellions
- Slavery and Abolition of Slavery
- Social and Cultural History
- Theory, Methods, and Historiography
- Urban History
- World History
- Browse content in Language Teaching and Learning
- Language Learning (Specific Skills)
- Language Teaching Theory and Methods
- Browse content in Linguistics
- Applied Linguistics
- Cognitive Linguistics
- Computational Linguistics
- Forensic Linguistics
- Grammar, Syntax and Morphology
- Historical and Diachronic Linguistics
- History of English
- Language Acquisition
- Language Evolution
- Language Reference
- Language Variation
- Language Families
- Lexicography
- Linguistic Anthropology
- Linguistic Theories
- Linguistic Typology
- Phonetics and Phonology
- Psycholinguistics
- Sociolinguistics
- Translation and Interpretation
- Writing Systems
- Browse content in Literature
Bibliography
- Children's Literature Studies
- Literary Studies (Asian)
- Literary Studies (European)
- Literary Studies (Eco-criticism)
- Literary Studies (Romanticism)
- Literary Studies (American)
- Literary Studies (Modernism)
- Literary Studies - World
- Literary Studies (1500 to 1800)
- Literary Studies (19th Century)
- Literary Studies (20th Century onwards)
- Literary Studies (African American Literature)
- Literary Studies (British and Irish)
- Literary Studies (Early and Medieval)
- Literary Studies (Fiction, Novelists, and Prose Writers)
- Literary Studies (Gender Studies)
- Literary Studies (Graphic Novels)
- Literary Studies (History of the Book)
- Literary Studies (Plays and Playwrights)
- Literary Studies (Poetry and Poets)
- Literary Studies (Postcolonial Literature)
- Literary Studies (Queer Studies)
- Literary Studies (Science Fiction)
- Literary Studies (Travel Literature)
- Literary Studies (War Literature)
- Literary Studies (Women's Writing)
- Literary Theory and Cultural Studies
- Mythology and Folklore
- Shakespeare Studies and Criticism
- Browse content in Media Studies
- Browse content in Music
- Applied Music
- Dance and Music
- Ethics in Music
- Ethnomusicology
- Gender and Sexuality in Music
- Medicine and Music
- Music Cultures
- Music and Religion
- Music and Media
- Music and Culture
- Music Education and Pedagogy
- Music Theory and Analysis
- Musical Scores, Lyrics, and Libretti
- Musical Structures, Styles, and Techniques
- Musicology and Music History
- Performance Practice and Studies
- Race and Ethnicity in Music
- Sound Studies
- Browse content in Performing Arts
- Browse content in Philosophy
- Aesthetics and Philosophy of Art
- Epistemology
- Feminist Philosophy
- History of Western Philosophy
- Metaphysics
- Moral Philosophy
- Non-Western Philosophy
- Philosophy of Science
- Philosophy of Language
- Philosophy of Mind
- Philosophy of Perception
- Philosophy of Action
- Philosophy of Law
- Philosophy of Religion
- Philosophy of Mathematics and Logic
- Practical Ethics
- Social and Political Philosophy
- Browse content in Religion
- Biblical Studies
- Christianity
- East Asian Religions
- History of Religion
- Judaism and Jewish Studies
- Qumran Studies
- Religion and Education
- Religion and Health
- Religion and Politics
- Religion and Science
- Religion and Law
- Religion and Art, Literature, and Music
- Religious Studies
- Browse content in Society and Culture
- Cookery, Food, and Drink
- Cultural Studies
- Customs and Traditions
- Ethical Issues and Debates
- Hobbies, Games, Arts and Crafts
- Lifestyle, Home, and Garden
- Natural world, Country Life, and Pets
- Popular Beliefs and Controversial Knowledge
- Sports and Outdoor Recreation
- Technology and Society
- Travel and Holiday
- Visual Culture
- Browse content in Law
- Arbitration
- Browse content in Company and Commercial Law
- Commercial Law
- Company Law
- Browse content in Comparative Law
- Systems of Law
- Competition Law
- Browse content in Constitutional and Administrative Law
- Government Powers
- Judicial Review
- Local Government Law
- Military and Defence Law
- Parliamentary and Legislative Practice
- Construction Law
- Contract Law
- Browse content in Criminal Law
- Criminal Procedure
- Criminal Evidence Law
- Sentencing and Punishment
- Employment and Labour Law
- Environment and Energy Law
- Browse content in Financial Law
- Banking Law
- Insolvency Law
- History of Law
- Human Rights and Immigration
- Intellectual Property Law
- Browse content in International Law
- Private International Law and Conflict of Laws
- Public International Law
- IT and Communications Law
- Jurisprudence and Philosophy of Law
- Law and Politics
- Law and Society
- Browse content in Legal System and Practice
- Courts and Procedure
- Legal Skills and Practice
- Primary Sources of Law
- Regulation of Legal Profession
- Medical and Healthcare Law
- Browse content in Policing
- Criminal Investigation and Detection
- Police and Security Services
- Police Procedure and Law
- Police Regional Planning
- Browse content in Property Law
- Personal Property Law
- Study and Revision
- Terrorism and National Security Law
- Browse content in Trusts Law
- Wills and Probate or Succession
- Browse content in Medicine and Health
- Browse content in Allied Health Professions
- Arts Therapies
- Clinical Science
- Dietetics and Nutrition
- Occupational Therapy
- Operating Department Practice
- Physiotherapy
- Radiography
- Speech and Language Therapy
- Browse content in Anaesthetics
- General Anaesthesia
- Neuroanaesthesia
- Browse content in Clinical Medicine
- Acute Medicine
- Cardiovascular Medicine
- Clinical Genetics
- Clinical Pharmacology and Therapeutics
- Dermatology
- Endocrinology and Diabetes
- Gastroenterology
- Genito-urinary Medicine
- Geriatric Medicine
- Infectious Diseases
- Medical Toxicology
- Medical Oncology
- Pain Medicine
- Palliative Medicine
- Rehabilitation Medicine
- Respiratory Medicine and Pulmonology
- Rheumatology
- Sleep Medicine
- Sports and Exercise Medicine
- Clinical Neuroscience
- Community Medical Services
- Critical Care
- Emergency Medicine
- Forensic Medicine
- Haematology
- History of Medicine
- Browse content in Medical Dentistry
- Oral and Maxillofacial Surgery
- Paediatric Dentistry
- Restorative Dentistry and Orthodontics
- Surgical Dentistry
- Browse content in Medical Skills
- Clinical Skills
- Communication Skills
- Nursing Skills
- Surgical Skills
- Medical Ethics
- Medical Statistics and Methodology
- Browse content in Neurology
- Clinical Neurophysiology
- Neuropathology
- Nursing Studies
- Browse content in Obstetrics and Gynaecology
- Gynaecology
- Occupational Medicine
- Ophthalmology
- Otolaryngology (ENT)
- Browse content in Paediatrics
- Neonatology
- Browse content in Pathology
- Chemical Pathology
- Clinical Cytogenetics and Molecular Genetics
- Histopathology
- Medical Microbiology and Virology
- Patient Education and Information
- Browse content in Pharmacology
- Psychopharmacology
- Browse content in Popular Health
- Caring for Others
- Complementary and Alternative Medicine
- Self-help and Personal Development
- Browse content in Preclinical Medicine
- Cell Biology
- Molecular Biology and Genetics
- Reproduction, Growth and Development
- Primary Care
- Professional Development in Medicine
- Browse content in Psychiatry
- Addiction Medicine
- Child and Adolescent Psychiatry
- Forensic Psychiatry
- Learning Disabilities
- Old Age Psychiatry
- Psychotherapy
- Browse content in Public Health and Epidemiology
- Epidemiology
- Public Health
- Browse content in Radiology
- Clinical Radiology
- Interventional Radiology
- Nuclear Medicine
- Radiation Oncology
- Reproductive Medicine
- Browse content in Surgery
- Cardiothoracic Surgery
- Gastro-intestinal and Colorectal Surgery
- General Surgery
- Neurosurgery
- Paediatric Surgery
- Peri-operative Care
- Plastic and Reconstructive Surgery
- Surgical Oncology
- Transplant Surgery
- Trauma and Orthopaedic Surgery
- Vascular Surgery
- Browse content in Science and Mathematics
- Browse content in Biological Sciences
- Aquatic Biology
- Biochemistry
- Bioinformatics and Computational Biology
- Developmental Biology
- Ecology and Conservation
- Evolutionary Biology
- Genetics and Genomics
- Microbiology
- Molecular and Cell Biology
- Natural History
- Plant Sciences and Forestry
- Research Methods in Life Sciences
- Structural Biology
- Systems Biology
- Zoology and Animal Sciences
- Browse content in Chemistry
- Analytical Chemistry
- Computational Chemistry
- Crystallography
- Environmental Chemistry
- Industrial Chemistry
- Inorganic Chemistry
- Materials Chemistry
- Medicinal Chemistry
- Mineralogy and Gems
- Organic Chemistry
- Physical Chemistry
- Polymer Chemistry
- Study and Communication Skills in Chemistry
- Theoretical Chemistry
- Browse content in Computer Science
- Artificial Intelligence
- Computer Architecture and Logic Design
- Game Studies
- Human-Computer Interaction
- Mathematical Theory of Computation
- Programming Languages
- Software Engineering
- Systems Analysis and Design
- Virtual Reality
- Browse content in Computing
- Business Applications
- Computer Security
- Computer Games
- Computer Networking and Communications
- Digital Lifestyle
- Graphical and Digital Media Applications
- Operating Systems
- Browse content in Earth Sciences and Geography
- Atmospheric Sciences
- Environmental Geography
- Geology and the Lithosphere
- Maps and Map-making
- Meteorology and Climatology
- Oceanography and Hydrology
- Palaeontology
- Physical Geography and Topography
- Regional Geography
- Soil Science
- Urban Geography
- Browse content in Engineering and Technology
- Agriculture and Farming
- Biological Engineering
- Civil Engineering, Surveying, and Building
- Electronics and Communications Engineering
- Energy Technology
- Engineering (General)
- Environmental Science, Engineering, and Technology
- History of Engineering and Technology
- Mechanical Engineering and Materials
- Technology of Industrial Chemistry
- Transport Technology and Trades
- Browse content in Environmental Science
- Applied Ecology (Environmental Science)
- Conservation of the Environment (Environmental Science)
- Environmental Sustainability
- Environmentalist Thought and Ideology (Environmental Science)
- Management of Land and Natural Resources (Environmental Science)
- Natural Disasters (Environmental Science)
- Nuclear Issues (Environmental Science)
- Pollution and Threats to the Environment (Environmental Science)
- Social Impact of Environmental Issues (Environmental Science)
- History of Science and Technology
- Browse content in Materials Science
- Ceramics and Glasses
- Composite Materials
- Metals, Alloying, and Corrosion
- Nanotechnology
- Browse content in Mathematics
- Applied Mathematics
- Biomathematics and Statistics
- History of Mathematics
- Mathematical Education
- Mathematical Finance
- Mathematical Analysis
- Numerical and Computational Mathematics
- Probability and Statistics
- Pure Mathematics
- Browse content in Neuroscience
- Cognition and Behavioural Neuroscience
- Development of the Nervous System
- Disorders of the Nervous System
- History of Neuroscience
- Invertebrate Neurobiology
- Molecular and Cellular Systems
- Neuroendocrinology and Autonomic Nervous System
- Neuroscientific Techniques
- Sensory and Motor Systems
- Browse content in Physics
- Astronomy and Astrophysics
- Atomic, Molecular, and Optical Physics
- Biological and Medical Physics
- Classical Mechanics
- Computational Physics
- Condensed Matter Physics
- Electromagnetism, Optics, and Acoustics
- History of Physics
- Mathematical and Statistical Physics
- Measurement Science
- Nuclear Physics
- Particles and Fields
- Plasma Physics
- Quantum Physics
- Relativity and Gravitation
- Semiconductor and Mesoscopic Physics
- Browse content in Psychology
- Affective Sciences
- Clinical Psychology
- Cognitive Psychology
- Cognitive Neuroscience
- Criminal and Forensic Psychology
- Developmental Psychology
- Educational Psychology
- Evolutionary Psychology
- Health Psychology
- History and Systems in Psychology
- Music Psychology
- Neuropsychology
- Organizational Psychology
- Psychological Assessment and Testing
- Psychology of Human-Technology Interaction
- Psychology Professional Development and Training
- Research Methods in Psychology
- Social Psychology
- Browse content in Social Sciences
- Browse content in Anthropology
- Anthropology of Religion
- Human Evolution
- Medical Anthropology
- Physical Anthropology
- Regional Anthropology
- Social and Cultural Anthropology
- Theory and Practice of Anthropology
- Browse content in Business and Management
- Business Strategy
- Business Ethics
- Business History
- Business and Government
- Business and Technology
- Business and the Environment
- Comparative Management
- Corporate Governance
- Corporate Social Responsibility
- Entrepreneurship
- Health Management
- Human Resource Management
- Industrial and Employment Relations
- Industry Studies
- Information and Communication Technologies
- International Business
- Knowledge Management
- Management and Management Techniques
- Operations Management
- Organizational Theory and Behaviour
- Pensions and Pension Management
- Public and Nonprofit Management
- Strategic Management
- Supply Chain Management
- Browse content in Criminology and Criminal Justice
- Criminal Justice
- Criminology
- Forms of Crime
- International and Comparative Criminology
- Youth Violence and Juvenile Justice
- Development Studies
- Browse content in Economics
- Agricultural, Environmental, and Natural Resource Economics
- Asian Economics
- Behavioural Finance
- Behavioural Economics and Neuroeconomics
- Econometrics and Mathematical Economics
- Economic Systems
- Economic History
- Economic Methodology
- Economic Development and Growth
- Financial Markets
- Financial Institutions and Services
- General Economics and Teaching
- Health, Education, and Welfare
- History of Economic Thought
- International Economics
- Labour and Demographic Economics
- Law and Economics
- Macroeconomics and Monetary Economics
- Microeconomics
- Public Economics
- Urban, Rural, and Regional Economics
- Welfare Economics
- Browse content in Education
- Adult Education and Continuous Learning
- Care and Counselling of Students
- Early Childhood and Elementary Education
- Educational Equipment and Technology
- Educational Strategies and Policy
- Higher and Further Education
- Organization and Management of Education
- Philosophy and Theory of Education
- Schools Studies
- Secondary Education
- Teaching of a Specific Subject
- Teaching of Specific Groups and Special Educational Needs
- Teaching Skills and Techniques
- Browse content in Environment
- Applied Ecology (Social Science)
- Climate Change
- Conservation of the Environment (Social Science)
- Environmentalist Thought and Ideology (Social Science)
- Natural Disasters (Environment)
- Social Impact of Environmental Issues (Social Science)
- Browse content in Human Geography
- Cultural Geography
- Economic Geography
- Political Geography
- Browse content in Interdisciplinary Studies
- Communication Studies
- Museums, Libraries, and Information Sciences
- Browse content in Politics
- African Politics
- Asian Politics
- Chinese Politics
- Comparative Politics
- Conflict Politics
- Elections and Electoral Studies
- Environmental Politics
- European Union
- Foreign Policy
- Gender and Politics
- Human Rights and Politics
- Indian Politics
- International Relations
- International Organization (Politics)
- International Political Economy
- Irish Politics
- Latin American Politics
- Middle Eastern Politics
- Political Methodology
- Political Communication
- Political Philosophy
- Political Sociology
- Political Behaviour
- Political Economy
- Political Institutions
- Political Theory
- Politics and Law
- Public Administration
- Public Policy
- Quantitative Political Methodology
- Regional Political Studies
- Russian Politics
- Security Studies
- State and Local Government
- UK Politics
- US Politics
- Browse content in Regional and Area Studies
- African Studies
- Asian Studies
- East Asian Studies
- Japanese Studies
- Latin American Studies
- Middle Eastern Studies
- Native American Studies
- Scottish Studies
- Browse content in Research and Information
- Research Methods
- Browse content in Social Work
- Addictions and Substance Misuse
- Adoption and Fostering
- Care of the Elderly
- Child and Adolescent Social Work
- Couple and Family Social Work
- Developmental and Physical Disabilities Social Work
- Direct Practice and Clinical Social Work
- Emergency Services
- Human Behaviour and the Social Environment
- International and Global Issues in Social Work
- Mental and Behavioural Health
- Social Justice and Human Rights
- Social Policy and Advocacy
- Social Work and Crime and Justice
- Social Work Macro Practice
- Social Work Practice Settings
- Social Work Research and Evidence-based Practice
- Welfare and Benefit Systems
- Browse content in Sociology
- Childhood Studies
- Community Development
- Comparative and Historical Sociology
- Economic Sociology
- Gender and Sexuality
- Gerontology and Ageing
- Health, Illness, and Medicine
- Marriage and the Family
- Migration Studies
- Occupations, Professions, and Work
- Organizations
- Population and Demography
- Race and Ethnicity
- Social Theory
- Social Movements and Social Change
- Social Research and Statistics
- Social Stratification, Inequality, and Mobility
- Sociology of Religion
- Sociology of Education
- Sport and Leisure
- Urban and Rural Studies
- Browse content in Warfare and Defence
- Defence Strategy, Planning, and Research
- Land Forces and Warfare
- Military Administration
- Military Life and Institutions
- Naval Forces and Warfare
- Other Warfare and Defence Issues
- Peace Studies and Conflict Resolution
- Weapons and Equipment

- < Previous chapter
- Next chapter >
27 Obesity and Responsibility
Beth Dixon is Professor of Philosophy at S.U.N.Y College at Plattsburgh.
- Published: 11 January 2018
- Cite Icon Cite
- Permissions Icon Permissions
This chapter explores whether obese individuals are morally responsible for their condition of obesity. The main argument is that some who are classified as obese are exempt from moral responsibility for two possible reasons. Either food situationism may interfere with an individual’s capacity to detect the moral considerations that favor healthy eating. Or, structural inequalities may interfere with an individual’s capacity to act on moral considerations that favor healthy eating. The account of situated moral agency employed here makes it possible to resist the false dichotomy of saying that either all obese individuals are morally responsible for being obese or that they are exempt from responsibility altogether. If moral exemptions apply in the way suggested, then a large number of individuals who are obese do not deserve to be the targets of moral blame, nor do they deserve the moral indignation that is sometimes directed toward them.
Introduction
There is almost no accounting for personal responsibility. People should be (and I believe they are) capable of not consuming everything the market throws their way. — Julie Guthman, Weighing In: Obesity, Food Justice, and the Limits of Capitalism 1
In this essay, I take a closer look at what personal responsibility means in connection to the “problem” of obesity and recommended solutions. 2 What we find in obesity discourse is that the language of personal responsibility sometimes has a moral dimension to it; although the attribution of moral responsibility rarely comes equipped with any clear criteria of application. This is true across a wide range of settings where the expression ‘personal responsibility’ is employed by academics, policy analysts, representatives of the food industry, or by ordinary citizens. This supplies us with sufficient rationale for engaging in a conceptual analysis of moral responsibility and how it applies in these contexts. As I will argue, such an analysis reveals that many who are classified as obese are actually exempt from moral responsibility, contrary to popular opinion.
A second reason for demanding clarity about the concept of moral responsibility as it applies to obesity discourse is that we may be able to use such an account to resist a false dichotomy about moral agency. 3 A prevalent idea about responsibility and obesity seems to suggest one of two possibilities. Either individuals are unequivocally responsible for their condition of being obese or individuals are excused from moral accountability because their condition of obesity is owed primarily to external conditions, namely, the “toxic” food environment, social institutions, public policy, the corporate food industry, or more fundamental unjust structural conditions. 4 As an example of the first position, when defenders of freedom of choice resist the regulation of processed foods and foods high in salt, sugar, and fat, they assume a much too expansive and liberal account of moral agency. They suppose (or want to convince us) that individual consumers already enjoy complete knowledge about the health dangers of processed food, and that they have an ideal kind of freedom to choose what to eat and how much to eat. 5 However, it is more realistic to suppose that moral agents are actually embedded in situations that, to a greater or lesser degree, constrain their knowledge of ethically salient features of the world which influence the control they have over their actions. Alternatively, when basic structural features of the world are implicated as part of a causal explanation for obesity, we are better able to focus on those social and political background conditions that disadvantage populations of people. 6 These contexts, to a greater or lesser degree, limit a person’s access to knowledge and create obstacles to eating healthy food. But, by exclusively emphasizing these structural conditions, it is easy to lose sight of the agency of individuals; what they know and how they can choose to act within the spheres of opportunity open to them. To capture this more realistic idea we should try to formulate a precise way of describing the kind of situated moral agency of individuals that continues to operate even in circumstances that constrain choices and limit opportunities. 7
A practically useful theory of moral responsibility should allow us to apply this account to the case study of obesity. Such an account should do the following: (1) identify what features of individuals matter for assessing moral responsibility. This should include what kinds of conditions count as exemptions from responsibility and blame; (2) allow us to say something specific about environmental circumstances that are salient to the issue of obesity. Since the food environment plays a significant role in discussions about the causes of and solutions to obesity, our theory of moral responsibility should be sensitive to features of these contextual background conditions; (3) specify the relevant kind of individual agency that makes sense of our way of talking about persons who are capable of giving reasons for what they do, and who are capable of exhibiting the relevant kind of control over their actions; and (4) identify a way of extending responsibility ascriptions beyond individual agents to collectives who may be suitable targets for moral blame as institutional or corporate “players” that contribute significantly to producing obesity in particular populations.
Here I employ a particular theory of moral responsibility formulated by Manuel Vargas in order to explain what it means to say that an individual is morally responsible for being obese (or not). 8 Vargas holds what he calls a “revisionist reasons” account of moral responsibility. 9 What is central to reasons accounts, in general, is that in order for a moral agent to be morally responsible for an action she performs, she must have the capacity to respond to reasons. 10 First, she must be capable of having the relevant kind of knowledge about herself and the world to recognize good reasons for acting. And second, she must be capable of responding to reasons by exerting the relevant kind of freedom and control over her actions. In other words, the agent must have the capacity to translate these reasons into motivations for acting and successfully perform an action based on these reasons. I will not argue for Vargas’s theory, per se, but I believe that it is independently plausible and, furthermore, possesses suitable resources for addressing the complexity of the case study of obesity. 11 This is so because it allows us to include in our assessment of individual responsibility those particular features of the environment that are relevant to an individual’s knowledge about, and control over, what she eats. This kind of situated agency is important for preserving our intuitions about how and why people act in practical and real world settings. 12
Finding Fault
In ordinary discourse about obesity and personal responsibility, we can detect a moral complaint about those who are obese and how they came to be that way. Consider the following student comments as reported by Guthman:
I think the people who eat the fast food are to blame. It is their choice to pull up to the drive-through, or to “supersize” their meal . . . . Although I agree that advertising and the food industry is partly at fault for advertising snack foods, I still feel that it is ultimately an individual choice to eat these foods. It basically comes down to will power. There are always temptations in life, but that doesn’t mean we have to go after those temptations. 13
In this context, what personal responsibility means is not merely that an obese person is the proximate cause of her condition, but that she bears some moral responsibility for those actions that lead to being obese. A related moral criticism takes the form of impugning the obese person’s moral character as intemperate (excessive in appetitive desires), lacking in self-discipline, or lazy. On this view, it might be thought that individuals who are obese are morally responsible for their condition because they have not tried hard enough, or simply have not opted to live in a healthy way. One of Guthman’s students articulates the concern this way:
I believe in this day and age, people know exactly what they are eating. . . . [M]y argument is that people do know, many times they simply choose not to live healthy lifestyles, and this is the major cause of obesity. 14
In other words, choosing not to improve oneself or to live a healthy lifestyle is reason to morally fault the character of an individual person for poor choices over a long period of time.
Perhaps the ideal target of these moral criticisms about unhealthy eating is a person I will call “Alex.” Alex is determined to adopt a healthier lifestyle. She believes that she can do so by limiting her consumption of salty, sugary, and fatty foods, exercising more by riding her bike, walking to work, and by attending a weekly Zumba class at the gym where she is a member. As part of her research about nutrition, Alex learns that a 12 oz. can of Coke or Pepsi contains 9 teaspoons of sugar. Because of this bit of knowledge, she comes to believe that soda is not part of a healthy diet. She forms the intention to avoid buying and consuming soda despite her desire to do so. Nonetheless, on a particular occasion in context C1 , Alex is out to lunch with her friends at Applebee’s and she orders a Coke to go with her salad. Is Alex morally responsible for this action in context C1 ? Applying a particular theory of responsibility to this basic illustrative example about Alex can help us see how to answer this question more precisely.
A Theory of Moral Responsibility
We might plausibly begin by saying that an individual person is morally responsible for her condition of obesity only if she has the knowledge to make informed choices as well as the relevant kind of freedom and control over her actions. But most of us will see straight away that knowledge, freedom, control, and choice are highly contestable philosophical concepts that require some definitional precision in order to be put to use in a convincing way. If we are to make distinctions in ascribing responsibility, then we must try to specify how the two central concepts of knowledge and control function as conditions for individual responsibility for action. Beyond being obese, there are many features about individuals and their circumstances that we will want to know more about when we apply the concepts of knowledge, control, and freedom of choice.
Consider how Vargas formulates the following conditions for responsible agency (RA):
(RA) An agent S is a responsible agent with respect to considerations of type M in circumstances C if S possesses a suite of basic agential capacities implicated in effective self-directed agency (including, for example, beliefs, desires, intentions, instrumental reasoning, and generally reliable beliefs about the world and the consequences of action) and is also possessed of the relevant capacity for (A) detection of suitable moral considerations M in C and (B) self-governance with respect to M in C . 15
(RA) captures a basic intuition about responsible agency. In order to be morally responsible for an action, agents must be capable of knowing and understanding morally relevant reasons for acting and also be capable of successfully acting on these moral reasons by exhibiting self-governance or volitional control. The epistemic and control conditions in (A) and (B) are further explained by specifying that the capacity for detection and self-governance may be realized in (i) the actual world, or in (ii) possible worlds where the agent is in a context “relevantly similar” to context C , and, in a suitable number of these worlds, the agent will successfully detect the relevant moral considerations and acquire the motivation to act accordingly, and does successfully act accordingly (214). I examine conditions (A) and (B) more carefully in subsequent sections.
What is interestingly different about (RA) compared to other reasons accounts of responsibility is that moral agents are judged responsible (or not) based on satisfying the detection and self-governance conditions in a particular set of circumstances, C . By adopting what he calls “circumstantialism” about capacities, Vargas thus rejects some standard assumptions that characterize other accounts of responsibility. One is the idea that agents are the kinds of beings that have free will because they have an intrinsic feature or property like a real self or rationality, which may be characterized as a “cross-situationally stable mechanism” specifiable in isolation from the agent’s external social or physical environment. This more standard view about responsibility allows us to say, for example, that both infants and schizophrenics are exempt from responsibility, presumably, because they lack this global and intrinsic ability to reason. Instead Vargas recommends that we conceive of responsible agency as a local and context-sensitive capacity that is realized (or not) in actual or possible situations. In other words, our rational capacities and our capacities for self-governance are not enjoyed independently of circumstances and situations, but are contingent on these circumstances. 16
In order to illustrate how to use and apply (RA), let us return to hypothetical Alex in our basic example. Is Alex morally responsible for her action in context C1 —consuming the Coke? Alex appears to satisfy condition (A) having the capacity for detecting relevant moral considerations M in circumstances C . The morally relevant considerations M in this example likely include: Alex’s intention to adopt a healthier lifestyle, her belief that eating nutritional food contributes to that goal, the particular knowledge Alex has about the sugar content in soda, and her belief that she ought to avoid drinking soda if she wants to lose weight and to live a healthier lifestyle. Does Alex satisfy condition (B) having the capacity for volitional control or self-governance with respect to the moral considerations M in circumstances C1 ? Let us suppose that Alex is sufficiently aware of these moral considerations at the time she is ordering lunch such that she is motivated to pursue a course of action that these moral considerations favor. Even though Alex seems to satisfy the detection condition in (RA), she fails to perform the action that these moral considerations favor (not buying the soda). The reason why this does not exempt her from moral responsibility is that there may be “relevantly similar” contexts in which Alex exercises the capacity for volitional control. Let’s pursue the matter just a bit further.
Later that week Alex finds herself in a different setting C2 at the grocery store to do her weekly shopping. At this time, it would seem that Alex is in a context “relevantly similar” to C1 the restaurant. At the grocery store, Alex continues to recognize and to endorse all of the relevant moral considerations cited previously in C1 about the value of health, the importance of eating nutritional food, and the high sugar content of soda, in particular, the belief that she ought not to drink soda if she wants to lose weight and to become healthier. She remembers her resolution to purchase healthier food and avoids the soda aisle altogether. At this time, she does not buy a six-pack of Coke because she believes that in order to live a healthier lifestyle—a value she endorses—she ought not to drink sugary beverages. So, even though Alex does not exhibit volitional control or self-governance with respect to her action in C1 at the restaurant, we see that she is capable of doing so in a context that is relevantly similar to the restaurant setting; a context where she is also faced with the decision about whether to buy and to consume sugary drinks. And let us further suppose that there are a “suitable proportion” of contexts where Alex does detect the moral considerations cited, is motivated to act for those reasons, and acts accordingly. Hence, Alex is morally responsible for her action of purchasing the soda in the context C1 at Applebee’s in spite of what appears to be a temporary lack of control. 17 So far, so good. But for many other obese individuals, the circumstances that affect choices about what to eat, and how much, are more complicated. In the next section, I consider another example about “Joyce” whose circumstances make her a candidate for exemption from moral responsibility for two reasons; she fails to satisfy the detection condition of (RA), and she fails to satisfy the volitional control condition of (RA).
The Detection Condition
According to (RA), a moral agent’s responsibility may be compromised by circumstances in which the agent cannot detect the moral considerations that are relevant to the context in which she finds herself. Vargas states the detection condition of (RA) in the following way:
(A) The capacity for detection of the relevant moral considerations obtains when: i. S actually detects moral consideration of type M in C that are pertinent to actions available to S ; or ii. In those possible worlds where S is in a context relevantly similar to C , and moral considerations of type M are present in those contexts, in a suitable proportion of those worlds S successfully detects those considerations. 18
Intuitively, what (A) says is that moral agents have the capacity for detecting reasons for action by what relevant moral considerations they can detect in circumstances C of the actual world, or in relevantly similar circumstances of other possible worlds.
In this section, I explore reasons for believing that some situational conditions may well interfere with an agent’s ability to detect moral considerations connected to buying and consuming unhealthy food. I call this “food situationism.” Food situationism is made plausible by reference to a body of social psychology research known as “situationist” research. Let us start with a representative example from the situationist literature, and then consider how food situationism might interfere with detecting the moral considerations relevant to buying and consuming unhealthy food.
One rather well-known example of the situationist research is called “Good Samaritan.” 19 John Darley and Daniel Batson tested seminary students on their proclivity to help a stranger in need. Groups of students were instructed to either prepare a talk on occupations for seminary students or to prepare a talk on the Good Samaritan parable. All groups were subsequently told to walk to another location to present their talks to an audience. But, in some cases, students were informed that they were late for their presentations and needed to hurry to the next building. The findings from this experiment revealed that the late students were less likely to help a citizen (experimenter) in clear view slumped in a hallway who appeared to need medical assistance. 20
How exactly does this kind of research apply to reasons accounts of moral responsibility, in particular? 21 One threat to responsibility that situationism seems to create is an epistemic one. Agents in situationist experiments seem to lack knowledge about the situational factors that affect their choices and behaviors. If agents in situationist experiments fail to see the situational factors that influence their behavior, then they do not act for reasons that they themselves can identify. 22 More problematically, they may well act for bad reasons. In his review and analysis of the situationist literature Vargas comes to a similar conclusion. Vargas agrees that there is a genuine threat to reasons accounts of responsibility because the “situational inputs” influence the agent’s behavior and actions but without the agent’s awareness of these situational factors. In other words, the agent’s deliberation and decision is irrelevant or non-operative in the production of action. And if it is the context and situation that predicts and explains the agent’s behavior instead, this suggests that “our agency is somewhat less than we presume.” 23 About the Good Samaritan, Vargas suggests that subjects may be described as suffering a “loss of capacity” to recognize moral reasons for helping. Specifically, subjects failed to see that someone needed help because of the situational forces operating at the time. Likewise, we might venture about food situationism that if agents cannot discern the relevant background conditions that influence their food choices, then this lack of knowledge interferes with acting on good reasons.
The ordinary consumer is not unfamiliar with the fact that the food industry devotes a great deal of time, money, and research into determining how best to influence our purchases. What perhaps is less well understood is the extent to which they are successful in producing environments that do influence our “choices.” 24 Background conditions exert a force on our consumption of unhealthy food by advertising the fact that processed food is cheap, available always and everywhere, as well as fast and convenient for busy people living busy lives. We are moved to buy bigger portions and to eat these larger amounts without understanding what situational factors influence this choice; from background music, price, and packaging, to disguised portion sizes and unspecified added amounts of sugar or calories. The “toxic environment” is more insidious still when it targets children by TV ads, cartoon characters, and by school districts buying into cafeteria fast-food outlets when educational resources are scarce. Food situationism includes all of these situational background conditions that affect what the consumer buys and eats. What impact does food situationism have on attributions of moral responsibility?
Suppose Joyce has only a short period of time before she starts her next shift at work. On her way, she stops at McDonald’s to order a “value-sized” meal that includes a Big Mac, large fries, and a 20 oz. Coke. Joyce does want to eat better food and believes that she should also lose weight (she is morbidly obese), but she has trouble implementing these desires and goals. Is Joyce morally responsible for buying and consuming unhealthy food on this occasion? Condition (A) directs our attention to Joyce’s capacity to detect moral considerations relevant to her action in C1 purchasing a McDonald’s meal. These moral considerations surely include her knowledge that the “value-sized” meal is not a healthy food choice. But it is not clear that this bit of general knowledge exhausts the content of what is morally relevant to her motivation to act.
Recall the seminary students in the research experiment, “Good Samaritan,” who failed to help an ailing confederate of the experiment who needed medical attention. What these students presumably could claim to know, if asked at any time during the experiment, is the general moral prescription that one ought to help those in need of medical attention. But in this case the seminary students failed to notice a particular moral consideration, namely, the need of the person they hurriedly passed. Dana Nelkin describes this failure as a local one when she conjectures that the seminary students failed to “pick up on morally salient features of the environment, a failure whose consequence is a failure to respond to reasons.” 25 Likewise, in C1 , Joyce may fail to see the particular moral considerations that bear on her purchasing the fast-food meal, even though she knows generally that it is unhealthy. For example, she does not know how many total calories she is consuming or how many calories overall she should be consuming per day. She does not know what counts as a “serving size” of fries, nor does she specifically know the nutritional content of what she consumes. In her experience at McDonald’s, there is nothing like a warning label that alerts her to these details (like the warning on a pack of cigarettes). The food is delivered to her quickly with a smiling Ronald beaming at her in the background. If we say that the seminary students are not responsible for failing to help a person in medical need because the situation unduly influenced their capacity to see and to detect the relevant moral considerations that included, “this person needs help,” then perhaps we should say about Joyce that she is not responsible for choosing to eat the fast-food meal. After all, she fails to see the particular circumstances that constitute the relevant moral considerations influencing her actions, not by the intentional design of a social psychologist researcher but by the intentional design of the food industry.
But additionally, according to (A)(ii), Joyce’s capacity to detect the moral considerations relevant to her action in C1 (purchasing and eating the “value” meal at McDonald’s) should be determined by whether she can detect these moral considerations in a suitable proportion of worlds or contexts that are relevantly similar to context C1 . In my hypothetical example, Joyce will also fail to detect particular facts about the nutritional content of what she eats in a large number of similar contexts where she is buying and consuming food. There are plausible reasons for this conjecture. One is that she is not devoted to learning about nutrition, per se. (Compare Alex who knows from her research exactly how many teaspoons of sugar are in a 12 oz. can of Coke.) Another reason why Joyce will probably not detect these moral considerations relevant to her favoring healthy food is that this information is hard to interpret and hard to understand in a wide variety of contexts; in the fast-food line or at a convenience store, or even at a large grocery store where, for example, the word “natural” applies to anything and everything, including processed food. Food situationism correctly describes most of the contexts in which Joyce buys and consumes unhealthy food. If the particular information that Joyce needs to make better food choices is opaque to her, then it would be unreasonable to hold Joyce morally responsible for eating unhealthy food.
It is important to include in this story about Joyce certain facts about why she is exempt from moral responsibility in context C1 and in a suitable proportion of worlds that are similar to C1 . This will be so when her failure to detect the relevant moral considerations is owed to deceptive advertising and marketing, or by manipulation of the situation in a suitable proportion of worlds that are similar to C1 ; the circumstances surrounding the purchase of a McDonald’s “value” meal. If these are the reasons that Joyce fails to have the capacity to detect moral considerations in favor of purchasing healthy food, then this failure of capacity is not owed to some obvious defect of her detection capacities overall. (RA) allows us to see that moral agents are situated in contexts that may well contribute to diminishing their capacities to detect relevant moral considerations. I believe that food situationism is one kind of context that degrades the epistemic capacities of Joyce and many other consumers who buy and consume unhealthy food. If so, then enhancing the epistemic capacities of Joyce, and other consumers like ourselves, involves changing the contexts that contribute to our abilities to detect the particular considerations in favor of eating healthy food. This point has obvious implications for obesity prevention policies, since we might emphasize that the circumstances that create obstacles to detecting what counts as a healthy food choice need to change, rather than the individual consumer herself. Policy recommendations that create enhanced conditions for detecting the relevant moral considerations about food choices might include, for example, better labeling of foods or improved regulation of deceptive marketing and advertising by the food industry.
Still, one might be tempted to say that Joyce’s (and others’) epistemic failure can be easily addressed. For example, Michael Moss recommends to the consumer to arm herself with knowledge as she confronts the grocery store “battlefield” riddled with landmines of salt, sugar, and fat in every aisle. 26 Moss rallies the consumer (soldier) by claiming that once we are armed with such knowledge about unhealthy ingredients, we have the power to make choices. This recommendation assumes that if the detection condition were satisfied in our hypothetical example, then Joyce could freely choose to eat healthy food. However, Joyce may not be able to translate knowledge about healthy food into motivations that lead to successfully buying and consuming healthy food. And this will be true for a large population of people who are obese but fail to have the capacity for self-governance through no fault of their own. I discuss these additional circumstances in the next section.
The Volitional Control Condition
It is sometimes argued that what may count as a moral excuse for blaming some individual eaters for being obese is that their freedom to choose healthy food is diminished when certain environmental conditions constrain and limit food choices. These conditions connected to diminished freedom and choice include lack of access to healthy and nutritious food (no transportation or limited mobility), prohibitive cost of healthy food, little time to cook meals at home, absence of retail grocery stores, and so on, in combination with the ubiquitous presence of unhealthy fast food both in schools and in low-income neighborhoods. 27 To explore the issue of diminished freedom and control, we might ask: Does Joyce have the capacity for volitional control to be held morally responsible for eating unhealthy food? Vargas specifies the conditions for this capacity in the following way:
(B) The capacity for volitional control, or self-governance with respect to the relevant moral considerations M in circumstances C obtains when either: i. S is, in light of awareness of M in C , motivated to accordingly pursue courses of action for which M counts in favor, and to avoid courses of action disfavored by M ; or ii. When S is not so motivated, in a suitable proportion of those worlds where S is in a context relevantly similar to C a. S detects moral considerations of type M , and b. in virtue of detecting M considerations, S acquires the motivation to act accordingly, and c. S successfully acts accordingly. 28
Intuitively, what (B) says is that moral agents have the capacity for volitional control if either these agents are motivated to act on relevant moral considerations in a context C of the actual world, or agents can successfully act on these moral considerations in possible contexts that are relevantly similar to C .
In circumstances C1 where Joyce buys and eats the “value” meal at McDonald’s, she is generally aware that the food is unhealthy, but she buys it anyway. We have considered the way in which food situationism might operate here, effectively interfering with her detection of the particular moral considerations that favor resisting the temptation for the fast-food meal. But condition (B)(ii) alerts us to other obstacles that might interfere with Joyce’s successfully making healthy choices about food. Even though Joyce is not motivated to act in accordance with moral considerations M in C1 , there may be other similar worlds or contexts ( C2, C3 . . .) where Joyce is faced with choices about what to eat, and she chooses to buy and eat healthy food. If so, then Joyce would demonstrate that she has the capacity for volitional control and, hence, that she is morally responsible for her action in C1 .
However, in this hypothetical example the contexts that are relevantly similar to C1 also prevent Joyce from successfully acting in accordance with her motivation to eat healthy food. This is so for a number of reasons. Consider these additional facts about Joyce and how she lives. Joyce is a single mother of two young children. She works long hours at two part-time jobs that pay minimum wage and which barely cover her monthly expenses for herself and her family. Additionally, she cannot afford a car, and she has no easy transportation to retail grocery stores. She uses public transportation that requires her to travel by bus on several routes to a larger shopping center. This means that most of the time she must shop for food at a corner convenience store and gas station that stocks mostly processed food, or she is able to buy quick cheap meals at the many fast-food restaurants that populate her neighborhood. In other words, even if Joyce were able to detect the relevant moral considerations that favor the action of purchasing healthy food, she would be unable to successfully act accordingly because in a suitable proportion of similar contexts she is constrained by mobility, access, cost, time, and the lack of other resources. This means that with respect to her purchase and consumption of the McDonald’s meal at C1 , Joyce has not satisfied condition (B)(ii) the capacity for volitional control in the circumstances described. So she is exempt from moral responsibility for her food choice in that context.
An Objection
A recent issue of Parade magazine was devoted to the popular TV reality show, The Biggest Loser . 29 In the accompanying article, this year’s trainers (Jen, Bob, and Dolvett) recommend various ways to lose weight by resisting temptation. Some of these “temptation busters” include: identifying and avoiding triggers to overeating, stocking your kitchen with only healthy foods, creating small exercise goals, and working out with a friend for extra motivation. There is nothing surprising here. In fact, these recommendations capture a very plausible intuition; we are in charge of our health. And if we just try hard enough, then we might be more successful in losing weight or adopting a healthier lifestyle. What is correct about this widespread belief is that the population of obese individuals consists of moral agents whose general capacities are intact for making free and informed choices. Nothing I have said about situated agency directly contradicts this very plausible idea. If so, a critic might insist about Joyce that she really does have the capacity for detecting moral considerations relevant to consuming healthy food, as well as the capacity for volitional control that results in her action of consuming healthy food. Since (RA) specifies that the detection and volitional control conditions are satisfied in possible worlds where the agent is in a “context relevantly similar to C ,” the challenge then is to say more about what it means for Joyce to satisfy the detection and control conditions in a “suitable proportion of relevantly similar contexts” to the actual circumstance of C1 (buying the “value” meal at McDonald’s). So what counts as a “relevantly similar context” to C1 ?
Let us imagine another context C2 that might be a suitable candidate for being a relevantly similar context to C1 . Suppose that in context C2 Joyce engages in research about nutrition to inform herself about the moral considerations relevant to purchasing healthy food. Maybe she reads about the “toxic environment” or even reads the definitive book on fast food, Fast Food Nation . 30 In this set of circumstances C2 , she understands in detail how environmental conditions or cues influence her eating behavior, and she also understands the poor nutritional quality of fast food. As a result, she chooses not to buy the value meal. If this is a relevantly similar context to C1 (and there are a sufficient number of these contexts), then Joyce does have the capacity for detection of moral considerations relevant to her choice of food.
Additionally, suppose that in context C2 there is a farmer’s market nearby and in that place fruits and vegetables are cheap and plentiful. In this context, Joyce would buy and make meals from this produce for healthy meals at home instead of buying dinner at McDonald’s. If this is a relevantly similar context to C1 (and there are a sufficient number of these contexts), then Joyce does demonstrate the capacity for volitional control, and in combination with satisfying condition (A)(ii) about the capacity for detection, it will be reasonable to suppose that she is morally responsible for her food choice at C1 . Are these circumstances described in C2 “relevantly similar” to the context C1 ?
To answer this question suppose we judge relevant similarity of context by imagining the number and kinds of facts about the actual world that must change in order to situate Joyce in the context C2 as described. 31 Here we should guard against oversimplifying the more general structural conditions that locate Joyce in C1 the actual world. Does Joyce have time to inform herself about the details of the nutritional quality of food she buys? Well, maybe if she did not work two part-time jobs. But this kind of employment is necessary for her because she is paid minimum wage. These jobs do not include health care insurance and her rent for housing comprises much of her monthly income. If Joyce did have a farmer’s market in her neighborhood, perhaps she might still not have the money or time to shop there and to prepare the food at home. Can she increase her earning potential so that she could afford to buy fresh produce? Only if she managed to attend college to retrain for other kinds of employment and only if there are sufficient jobs available in her area. But who would take care of her children and pay the rent while she was in school? And so on. These details are intended to remind the reader about the social, economic, and political distance between circumstances in C1 the actual world, and C2 the world in which Joyce is able to successfully act on moral considerations that favor healthy eating. The dissimilarity between these contexts is owed to poverty and inequality, and the relative distance in the “social and cultural circumstances of our agency” between C1 and C2 is vast. 32
What we should conclude is that Joyce’s situated agency is a function of fundamental structural conditions that include social and economic policies which create and sustain unequal opportunities in employment, education, health care, housing, and so on. These conditions limit choices and opportunities to function for populations or sub groups. As it turns out, (RA) and specifically condition (A)(ii) about the capacity for detection of moral considerations and condition (B)(ii) about the capacity for volitional control, are able to capture how an individual’s capacities for detection and volitional control are affected by these structural conditions. (RA) implies that individuals who occupy this social and political position are not morally responsible for their failure to eat healthy food as well as their condition of obesity if this is, in fact, a consequence of their food choices. They are like Joyce in this respect. But (RA) also allows us to say something intuitively plausible about the moral agency of Joyce and others that are similarly affected by structural inequalities. Individuals within this demographic may not be morally responsible for unhealthy eating. But their moral agency, in general, is not globally compromised by their social and political location since there are many kinds of actions they can perform in a variety of other contexts that satisfy the detection condition (A) and the volitional control condition (B) of (RA). What is wrong or, at least, misleading about the “temptation busters” recommendations is that by exclusively profiling the agent’s individual responsibility for resisting temptations we lose sight of the way in which agents are situated in circumstances that diminish the agent’s particular capacities for detection and control over healthy food choices. To reply to the critic, we should draw attention to these more fundamental structural conditions that degrade Joyce’s (and others’) capacity to detect moral considerations that favor purchasing healthy food, as well as her capacity for volitional control that results in successfully buying and consuming healthy foods. For some obese people, like Joyce, the temptation buster’s recommendations will be ineffectual; but not because they have not tried hard enough to resist temptation.
Extending the Scope of Responsibility
One advantage of employing the analysis of responsibility recommended by (RA) is to bring into clearer focus those background conditions that compromise moral agency. By seeing what contributes to diminished moral agency, we can more easily extend the scope of responsibility beyond individuals to institutions, policies, and corporate players.
In particular, it is important to recognize that societies, states, and cultures all structure our actual capacities. Being raised in an antiracist context plays a role in enhancing sensitivity to moral considerations tied to antiracist concerns. Similarly, being raised in a sexist, fascist, or classist culture will ordinarily shape a person’s incapacities to respond to egalitarian concerns. Such considerations may suggest that we need to ask whether societies or states have some kind of moral, practical, or political obligation to endeavor to shape the circumstances of actors in ways that insulate them against situational effects that degrade their (moral or other) reasoning. We might go on to ask whether societies or states have commensurate obligations to foster contexts that enhance our rational and moral agency. If they do, it suggests that free will is less a matter of science than it is of politics or morality. 33
Here Vargas asks a general rhetorical question about whether states and societies may be morally implicated in structuring our capacities to detect moral considerations and for self-governance. But the question has critical bite in the context of this real world issue about obesity. Institutions and states design and implement public health policies, allow for corporate manipulation of consumers by the food industry, tolerate fundamental inequities that sustain conditions of poverty and inequality (health care, education, housing, toxic food, and polluted environments, etc.). To the extent that these policies, corporate actors, and representatives of government create obstacles to moral agency, they are morally blameworthy. 34 Of course, this claim reaches beyond obesity discourse and obesity prevention policies. The point of demanding that such conditions be honored is to optimize the circumstances necessary for all moral agents to exercise their agency; not just those who are overweight.
Vargas uses the expression “moral architecture” to refer to the possibility of intentionally shaping and cultivating those conditions that structure our actual capacities that are conducive to responsible agency. 35 How might moral architecture be implemented in our particular study of obesity and responsibility? One insight from our discussion of food situationism is that moral agents need help in order to enhance their capacities to see the situations that influence their consumption of unhealthy food. Another epistemic obstacle specific to the discourse about obesity and responsibility is the general population’s inability to see and to understand how structural conditions circumscribe agency, and in some cases exempt individuals from moral responsibility. One mechanism for addressing both kinds of obstacles is what I have elsewhere called a “food justice narrative.” 36 These are stories that include the particular circumstances of a person’s life that illustrate how an individual is situated in, and influenced by, structural conditions that constrain choices and limit opportunities to act. This kind of story reminds us that particular populations of people retain their agency even as their choices are limited by the combined effect of these structural conditions. 37 In this context, the real explanatory value of such stories will be to reveal how our consumption of food is shaped by conditions that are largely unseen and undetected.
Let us return to the two main reasons for seeking greater clarity about how the concept of moral responsibility is used in obesity discourse. One rationale for doing so is that in these settings the concept of responsibility rarely comes equipped with any criteria of application. Now that we have introduced a revisionist reasons account of responsibility, we see how the knowledge and control conditions for being responsible can be used to decide how moral responsibility applies to obese populations. In previous sections, I have argued that Joyce is exempt from moral responsibility for two kinds of reasons. First, it is plausible to suppose that food situationism diminishes Joyce’s capacity to detect the considerations that favor buying and eating healthy food in a wide range of relevantly similar contexts. Second, Joyce’s social and political location contributes to undermining her capacity for volitional control in a wide range of contexts where she may recognize reasons for choosing to eat healthy food but cannot act accordingly. While not every individual who is obese can be exempted from moral responsibility for their food choices, hypothetical Joyce surely represents a large population of actual people who find themselves in a similar set of circumstances. What is significant about this conclusion is that contrary to what some believe, the property of being obese does not single out a class of individuals who are also morally responsible for their condition of obesity. Instead the way we determine attributions of responsibility is owed to (RA) where the relevant features are having the capacity to detect moral considerations relevant to action, and having the capacity for volitional control over the actions that these moral considerations favor. Additionally, attributions of responsibility are made about an agent’s capacities as these are exercised in actual and possible circumstances that are relevantly similar. So if moral exemptions apply in the way I have argued, then a large number of individuals who are obese do not deserve to be the targets of moral blame nor do they deserve the moral indignation that is sometimes directed toward them.
This account of situated agency also meets the second demand for the project undertaken here which is to resist the false dichotomy of saying either that individuals are morally responsible for being obese or that individuals are exempt from responsibility. Specifying and describing the circumstances of situated agents in judging attributions of responsibility allows us to include in our moral appraisal structural background conditions that limit knowledge and constrain freedoms and opportunities. But in doing so there is no need to choose between either holding a person morally responsible or blaming the food environment or structural conditions instead. The situated agency of individuals allows us to make this contextual analysis without forcing a choice between these two extreme positions about responsibility. In other words, (RA) offers us a more nuanced way of understanding how to assign moral responsibility to an agent who is situated in contexts that variously affect that agent’s ability to detect moral considerations and to act successfully in accordance with these moral considerations.
I conclude with the following disclaimer. Hypothetical “Joyce” only incompletely represents the lives of actual obese people who decide what to eat and attempt to act on their food choices. By this example, I do not pretend to capture all of the real world circumstances relevant to the moral appraisal of this population. Even so the analysis here suggests that we have sufficient theoretical resources to resist the presumption that all obese individuals are appropriate targets for moral disapprobation. 38
Arpaly, Nomy. Unprincipled Virtue: An Inquiry into Moral Agency . New York: Oxford University Press, 2003 .
Google Scholar
Google Preview
Asch, Solomon. “Effects of Group Pressures upon the Modification and Distortion of Judgment.” In Groups, Leadership, and Men , edited by Harold Guetzkow , 177–190. Pittsburgh, PA: Carnegie Press, 1951 .
Ashton, Alison. “The Temptation Busters.” Parade Magazine , January 3, 2016.
Barnhill, Anne , Katherine F. King , Nancy Kass , and Ruth Faden . “ The Value of Unhealthy Eating and the Ethics of Healthy Eating Policies. ” Kennedy Institute of Ethics Journal 24, no. 3 ( 2014 ): 187–217.
Benfarado, Adam , Jon Hanson , and David Yosifon . “ Broken Scales: Obesity and Justice in America. ” Emory Law Journal 53 (October 1, 2004): 1645–1806.
Brownell, Kelly D. , Rogan Kersh , David S. Ludwig , Robert C. Post , Rebecca M. Puhl , Marlene B. Schwartz , and Walter C. Willett . “ Personal Responsibility and Obesity: A Constructive Approach to a Controversial Issue. ” Health Affairs 29, no. 3 (March 2010): 378–386.
Ciurria, Michelle. “ Moral Responsibility Ain’t Just in the Head. ” Journal of the American Philosophical Association 1, no. 4 (Winter 2015 ): 601–616.
______. “ Situationism, Moral Responsibility and Blame. ” Philosophia 41 ( 2013 ): 179–193.
Clark, Andy , Julian Kiverstein , and Tillman Vierkant , eds. Decomposing the Will . Oxford: Oxford University Press, 2013 .
Crawford, Robert. “ Healthism and the Medicalization of Everyday Life. ” International Journal of Health Services 10, no. 3 ( 1980 ): 365–388.
______. “ You Are Dangerous to Your Health: The Ideology and Politics of Victim Blaming. ” International Journal of Health Services 7, no. 4 ( 1977 ): 663–680.
Darley, John , and Daniel Batson . “ ‘From Jerusalem to Jericho’: A Study of Situational and Dispositional Variables in Helping Behavior. ” Journal of Personality and Social Psychology 27 ( 1973 ): 100–108.
Dixon, Beth. “ Learning to See Food Justice. ” Agriculture and Human Values 31, no. 2 ( 2014 ): 175–184.
Fischer, John Martin , and Mark Ravizza . Responsibility and Control: A Theory of Moral Responsibility . Cambridge Studies in Philosophy and Law. Cambridge: Cambridge University Press, 1998 .
Guthman, Julie. Weighing In: Obesity, Food Justice, and the Limits of Capitalism . California Studies in Food and Culture. Berkeley and Los Angeles: University of California, 2011 .
Haney, Craig , Curtis Banks , and Philip Zimbardo . “ Interpersonal Dynamics in a Simulated Prison. ” International Journal of Criminology and Penology 1 ( 1973 ): 69–97.
Hartshorne, Hugh , and Mark May . Studies in the Nature of Character: Studies in Deceit . Vol. 1. New York: MacMillan, 1928 .
Isen, Alice , and Paula Levin . “ Effect of Feeling Good on Helping. ” Journal of Personality and Social Psychology 21 ( 1972 ): 384–388.
Kirkland, Anna. “ The Environmental Account of Obesity: A Case for Feminist Skepticism. ” Signs 36, no. 2 ( 2011 ): 463–485.
Knowles, John H. “The Responsibility of the Individual.” In Doing Better and Feeling Worse: Health in the United States , edited by John H. Knowles , 57–80. New York: W. W. Norton, 1977 .
Latane, Bibb , and Judith Rodin . “ A Lady in Distress: Inhibiting Effects of Friends and Strangers on Bystander Intervention. ” Journal of Experimental Social Psychology 5 ( 1969 ): 189–202.
Lyons, Pat. “Prescription for Harm: Diet Industry Influence, Public Health Policy, and the ‘Obesity Epidemic.’” In The Fat Studies Reader , edited by Esther Rothblum and Sondra Solovay , 75–87. New York: New York University Press, 2009 .
Mead, Lawrence M. Beyond Entitlement: The Social Obligations of Citizenship . New York: Free Press, 2006 .
Milgram, Stanley. “ Behavioral Study of Obedience. ” Journal of Abnormal and Social Psychology 67 ( 1963 ): 371–378.
Moss, Michael. Salt Sugar Fat: How the Food Giants Hooked Us . New York: Random House, 2013 .
Murray, Charles. Losing Ground: American Social Policy, 1950‒1980 . New York: Basic Books, 1984 .
Nelkin, Dana K. “ Freedom, Responsibility and the Challenge of Situationism. ” Midwest Studies in Philosophy 29 ( 2005 ): 181–206.
Nelson, Hilde Lindemann. Damaged Identities, Narrative Repair . Ithaca, NY: Cornell University Press, 2001 .
Nestle, Marian. Food Politics: How the Food Industry Influences Nutrition and Health . Berkeley and Los Angeles: University of California, 2002 .
Nussbaum, Martha. “Non-Relative Virtues: An Aristotelian Approach.” In The Quality of Life , edited by Martha Nussbaum and Amartya Sen , 242–269. Oxford: Clarendon Press, 1993 .
Schlosser, Eric. Fast Food Nation: The Dark Side of the All-American Meal . New York: HarperPerennial, 2005 .
Vargas, Manuel. Building Better Beings: A Theory of Moral Responsibility . New York: Oxford University Press, 2013 .
______. “Situationism and Moral Responsibility: Free Will in Fragments.” In Decomposing the Will , edited by Andy Clark , Julian Kiverstein , and Tillman Vierkant , 325–349. Oxford: Oxford University Press, 2013 .
Veatch, Robert M. “ Voluntary Risks to Health. ” Journal of the American Medical Association 243, no. 1 (January 4, 1980): 50–55.
Wallace, R. Jay. Responsibility and the Moral Sentiments . Cambridge, MA: Harvard University Press, 1994 .
Wansik, Brian. Mindless Eating: Why We Eat More Than We Think . New York: Bantam Books, 2006 .
Wikler, Daniel. “ Who Should Be Blamed for Being Sick? ” Health Education Quarterly 14, no. 1 (Spring 1987 ): 11–25.
Wolf, Susan. Freedom Within Reason . New York: Oxford University Press, 1990 .
Young, Iris Marion. Responsibility for Justice . Oxford Political Philosophy. Oxford: Oxford University Press, 2011 .
Zinczenko, David. “Don’t Blame the Eater.” New York Times. November 23, 2002, sec. Opinion.
Student comments as reported by Julie Guthman , Weighing In: Obesity, Food Justice, and the Limits of Capitalism , California Studies in Food and Culture (Berkeley and Los Angeles: University of California, 2011), 50–51
Identifying obesity as a “problem” (trend or epidemic) is itself contestable. See, e.g., Pat Lyons , “Prescription for Harm: Diet Industry Influence, Public Health Policy, and the ‘Obesity Epidemic,’” in The Fat Studies Reader , ed. Esther Rothblum and Sondra Solovay (New York: New York University Press, 2009), 75–87 ; Guthman, Weighing In ; and Kirkland, “The Environmental Account of Obesity : A Case for Feminist Skepticism.”
In Responsibility for Justice , Young makes a similar comment when she discusses personal responsibility in the context of public policy discourse about poverty and welfare reform. She criticizes Charles Murray and Lawrence Mead for assuming that individual responsibility and structural explanations of poverty are mutually exclusive explanations (17). Here I do not charge any one author with the same kind of mistake. What is still problematic is that emphasizing structural conditions in causal accounts of obesity risks understating or neglecting individual agency, which most of us believe continues to operate even when choices and opportunities are limited. See Charles Murray , Losing Ground: American Social Policy, 1950‒1980 (New York: Basic Books, 1984) ; and Lawrence M. Mead , Beyond Entitlement: The Social Obligations of Citizenship (New York: Free Press, 2006) .
See, e.g., Marian Nestle , Food Politics: How the Food Industry Influences Nutrition and Health (Berkeley and Los Angeles: University of California, 2002) ; and Kelly D. Brownell et al., “Personal Responsibility and Obesity: A Constructive Approach to a Controversial Issue,” Health Affairs 29, no. 3 (March 2010): 378–386 .
For example, consider what Congressman Ric Keller says in defense of the Personal Responsibility in Food Consumption Act.
We believe there should be common sense in a food court, not blaming other people in a legal court whenever there is an excessive consumption of fast food. . . . We think that most people understand that its common sense that if you eat unlimited amounts of supersize fries and milkshakes and Big Macs . . . that can possibly lead to obesity and things like diabetics [and] cardiovascular disease (quoted in Adam Benfarado, Jon Hanson, and David Yosifon, “Broken Scales : Obesity and Justice in America,” Emory Law Journal 53 [October 1, 2004]: 1645–1806).
See, e.g., Guthman, Weighing In ; and Kirkland, “The Environmental Account of Obesity : A Case for Feminist Skepticism.”
An additional rationale for seeking clarity about obesity and moral responsibility is that some kinds of obesity prevention policy recommendations may depend on targeting those populations of people who are believed to freely and knowingly undertake risks with their health. See, e.g., the discussion of fairness in Daniel Wikler , “Who Should Be Blamed for Being Sick?” Health Education Quarterly 14, no. 1 (Spring 1987): 11–25 ; and John H. Knowles , “The Responsibility of the Individual,” in Doing Better and Feeling Worse: Health in the United States , ed. John H. Knowles (New York: W. W. Norton, 1977), 57–80 ; Robert Crawford , “You Are Dangerous to Your Health: The Ideology and Politics of Victim Blaming,” International Journal of Health Services 7, no. 4 (1977): 663–680 ; Robert Crawford , “Healthism and the Medicalization of Everyday Life,” International Journal of Health Services 10, no. 3 (1980): 365–388 ; Robert M. Veatch , “Voluntary Risks to Health,” Journal of the American Medical Association 243, no. 1 (January 4, 1980): 50–55 .
Manuel Vargas , Building Better Beings: A Theory of Moral Responsibility (New York: Oxford University Press, 2013) ; Manuel Vargas , “Situationism and Moral Responsibility: Free Will in Fragments,” in Decomposing the Will , ed. Andy Clark , Julian Kiverstein , and Tillman Vierkant (Oxford: Oxford University Press, 2013), 325–349 .
The theory is “revisionist” in the sense that it requires relinquishing some common sense intuitions about responsibility. See Vargas, Building Better Beings: A Theory of Moral Responsibility , 2.
With some variation, the following views may qualify as reasons accounts: Susan Wolf , Freedom Within Reason (New York: Oxford University Press, 1990) ; R. Jay Wallace , Responsibility and the Moral Sentiments (Cambridge, MA: Harvard University Press, 1994) ; John Martin Fischer and Mark Ravizza , Responsibility and Control: A Theory of Moral Responsibility (New York: Cambridge University Press, 1998) ; Nomy Arpaly , Unprincipled Virtue: An Inquiry into Moral Agency (New York: Oxford University Press, 2003) ; Dana Nelkin , “Responsibility and Rational Abilities: Defending an Asymmetrical View,” Pacific Philosophical Quarterly 89 (2008): 497–515 .
See also Vargas’s motivations for adopting a reasons account in Building Better Beings , ch. 5, “The Primacy of Reasons,” 135–157.
Following Ciurria, we might classify Vargas’s account as “psychological externalism” about moral responsibility. See Michelle Ciurria , “Moral Responsibility Ain’t Just in the Head,” Journal of the American Philosophical Association 1, no. 4 (Winter 2015): 601–616 .
Guthman, Weighing In , 50–51.
Ibid. , 51 .
Vargas, Building Better Beings: A Theory of Moral Responsibility , 213–214.
For a more complete explanation of the standard features of reasons accounts that Vargas rejects (atomism and monism), see 204–209.
In order to keep this basic illustrative example relatively uncomplicated, I do not include a discussion about whether Alex is blameworthy for her action.
Vargas, Building Better Beings: A Theory of Moral Responsibility , 216.
John Darley and Daniel Batson , “‘From Jerusalem to Jericho’: A Study of Situational and Dispositional Variables in Helping Behavior,” Journal of Personality and Social Psychology 27 (1973): 100–108 .
Other similar experiments that comprise the situationist literature include: Stanford Prison Experiment ( Craig Haney , Curtis Banks , and Philip Zimbardo , “Interpersonal Dynamics in a Simulated Prison,” International Journal of Criminology and Penology 1 [1973]: 69–97 ); Honest School Children ( Hugh Hartshorne and Mark May , Studies in the Nature of Character: Studies in Deceit , vol. 1 [New York: MacMillan, 1928] ); Dime in the Phone Booth ( Alice Isen and Paula Levin , “Effect of Feeling Good on Helping,” Journal of Personality and Social Psychology 21 [1972]: 384–388 ); Helping Behavior in the Waiting Room ( Bibb Latane and Judith Rodin , “A Lady in Distress: Inhibiting Effects of Friends and Strangers on Bystander Intervention,” Journal of Experimental Social Psychology 5 [1969]: 189–202 ); Matching Lines ( Solomon Asch , “Effects of Group Pressures upon the Modification and Distortion of Judgment,” in Groups, Leadership, and Men , ed. Harold Guetzkow [Pittsburgh, PA: Carnegie Press, 1951], 177–190 ); and Shocking Behavior ( Stanley Milgram , “Behavioral Study of Obedience,” Journal of Abnormal and Social Psychology 67 [1963]: 371–378 ).
For a discussion of how situationism affects attributions of responsibility for virtues and vices of moral character, see Michelle Ciurria , “Situationism, Moral Responsibility and Blame,” Philosophia 41 (2013): 179–193 .
See, e.g., Dana K. Nelkin , “Freedom, Responsibility and the Challenge of Situationism,” Midwest Studies in Philosophy 29 (2005): 181–206 .
Vargas, “Situationism and Moral Responsibility: Free Will in Fragments,” 327.
Some social psychology research indicates that subjects will consume more if the container (popcorn, jelly beans, soda) is larger even though this is not a deliberate or conscious decision by the subject. See, e.g., Brian Wansik , “Environmental Factors That Increase the Food Intake and Consumption Volume of Unknowing Consumers,” Annual Review of Nutrition 24, no. 1 (2004): 455–479 ; Brian Wansik , Mindless Eating: Why We Eat More Than We Think (New York: Bantam Books, 2006) . This research suggest that agents are acting “non-autonomously” because they are motivated to consume more food but are doing so without being fully informed or without voluntarily choosing to consume more food. Barnhill et al. use this kind of example to explore whether policies designed to address obesity by limiting unhealthy eating count as justified paternalism. But the same kind of example is relevant to assessing whether agents are morally responsible. See Anne Barnhill et al., “The Value of Unhealthy Eating and the Ethics of Healthy Eating Policies,” Kennedy Institute of Ethics Journal 24, no. 3 (2014): 187–217 .
Nelkin, “Freedom, Responsibility and the Challenge of Situationism,” 204.
Michael Moss , Salt Sugar Fat: How the Food Giants Hooked Us (New York: Random House, 2013) .
See, e.g., David Zinczenko , “Don’t Blame the Eater,” New York Times , November 23, 2002 , sec. Opinion.
Vargas, Building Better Beings: A Theory of Moral Responsibility , 222–223.
Alison Ashton , “The Temptation Busters,” Parade Magazine , January 3, 2016 .
Eric Schlosser , Fast Food Nation: The Dark Side of the All-American Meal (New York: HarperPerennial, 2005) .
This is consistent with how Vargas explains judgments about similarity of contexts. See Vargas, Building Better Beings: A Theory of Moral Responsibility , 218–219.
Guthman makes a similar point in Weighing In , 196.
Vargas, “Situationism and Moral Responsibility: Free Will in Fragments,” 343.
In this case, the function of moral blame will be different than it is when directed to individual moral agents, since as Vargas remarks, institutions and collectives do not have “our ordinary capacities to recognize and respond to moral considerations” ( Vargas, Building Better Beings: A Theory of Moral Responsibility , 243).
Ibid. , 246–247 .
Beth Dixon , “Learning to See Food Justice,” Agriculture and Human Values 31, no. 2 (2014): 175–184 .
Vargas is sympathetic to using narratives in this way. He says,
How we conceive of our agency, and the powers we take agents to ordinarily have, will play some role in whether or not we are responsible agents in a given context, because of the power of such narratives to structure our agency. By promulgating narratives of control in those circumstances that test our control, we might (at least sometimes) make it the case that agents come to have enough self-control to be responsible agents. Similarly, by promulgating narratives of incapacity, of the inevitability of caving in to nigh-irresistible desires and temptations, we run the risk of self-fulfilling narratives here too (246).
The possible worries about narratives used in this way to shape agency is that some narratives may have built into them gender, racial, or class stereotypes that degrade individuals and their group identities. Hilde Lindemann Nelson calls these “master narratives.” See Hilde Lindemann Nelson , Damaged Identities, Narrative Repair (Ithaca, NY: Cornell University Press, 2001) .
My thanks to Anne Barnhill, Mark Bryant Budolfson, and Tyler Doggett for helpful comments on an earlier draft of this paper.
- About Oxford Academic
- Publish journals with us
- University press partners
- What we publish
- New features
- Open access
- Institutional account management
- Rights and permissions
- Get help with access
- Accessibility
- Advertising
- Media enquiries
- Oxford University Press
- Oxford Languages
- University of Oxford
Oxford University Press is a department of the University of Oxford. It furthers the University's objective of excellence in research, scholarship, and education by publishing worldwide
- Copyright © 2024 Oxford University Press
- Cookie settings
- Cookie policy
- Privacy policy
- Legal notice
This Feature Is Available To Subscribers Only
Sign In or Create an Account
This PDF is available to Subscribers Only
For full access to this pdf, sign in to an existing account, or purchase an annual subscription.
Obesity and responsibility: Is it time to rethink agency?
Affiliations.
- 1 Diabetes Complications Research Centre, Conway Institute, University College Dublin, Dublin, Ireland.
- 2 Department of Psychology, City Colleges, Dublin, Ireland.
- PMID: 33977636
- DOI: 10.1111/obr.13270
Despite obesity declared a disease, there still exists considerable weight stigma in both popular culture and health care, which negatively impacts policy making regarding prevention and treatment. While viewed as a choice or a failure of willpower by many, evidence exists to challenge the argument that both weight gain and failure to achieve weight loss maintenance are the individuals' fault due to personal failure or lack of responsibility. In this article, we draw upon literature from obesity treatment, neuroscience, philosophy of mind, and weight stigma to challenge the commonly held beliefs that individuals are free to choose how much they can weigh, and achievement of long-term weight loss maintenance is completely subject to conscious choice. In reality, the regulation of hunger, satiety, energy balance, and body weight takes place in subcortical regions of the brain. Thus, hunger and satiety signals are generated in regions of the brain, which are not associated with conscious experience. This points towards biological determinism of weight and challenges ideas of willpower and resultant moralization regarding body weight regulation. In this article, we will thus argue that in the context of dysregulation of hunger and satiety contributing to the obesity epidemic, a wider discourse related to personal responsibility and the stigma of obesity is needed to enhance understanding, prevention, and treatment of this complex disease. Obesity is a chronic disease requiring personalized treatment. Lifestyle interventions alone may not be enough to achieve medically significant and sustained weight loss for many individuals with obesity. By understanding that obesity is not due to a lack of motivation or willpower, the availability and utilization of additional treatments or combination of treatments such as lifestyle, pharmacotherapy, and surgery are likely to improve the quality of life for many suffering with this disease.
Keywords: conscious experience; obesity; responsibility; stigma.
© 2021 World Obesity Federation.
Publication types
- Obesity* / prevention & control
- Quality of Life*
- Weight Gain
- Weight Loss
- Share full article
Advertisement
Supported by
Guest Essay
Scientists Don’t Agree on What Causes Obesity, but They Know What Doesn’t

By Julia Belluz
Ms. Belluz is a health journalist. She is writing a book about nutrition and metabolism.
LONDON — A select group of the world’s top researchers studying obesity recently gathered in the gilded rooms of the Royal Society, the science academy of Isaac Newton and Charles Darwin, where ideas like gravity and evolution were once debated.
Now scientists were arguing about the causes of obesity, which affects more than 40 percent of U.S. adults and costs the health system about $ 173 billion each year . At the meeting’s closing session, John Speakman , a biologist, offered this conclusion on the subject: “There’s no consensus whatsoever about what the cause of it is.”
That’s not to say the researchers disagreed on everything. The three-day meeting was infused with an implicit understanding of what obesity is not: a personal failing. No presenter argued that humans collectively lost willpower around the 1980s, when obesity rates took off, first in high-income countries, then in much of the rest of the world. Not a single scientist said our genes changed in that short time. Laziness, gluttony and sloth were not referred to as obesity’s helpers. In stark contrast to a prevailing societal view of obesity, which assumes people have full control over their body size, they didn’t blame individuals for their condition, the same way we don’t blame people suffering from the effects of undernutrition, like stunting and wasting.
The researchers instead referred to obesity as a complex, chronic condition, and they were meeting to get to the bottom of why humans have, collectively , grown larger over the past half century. To that end, they shared a range of mechanisms that might explain the global obesity surge. And their theories, however diverse, made one thing obvious: As long as we treat obesity as a personal responsibility issue, its prevalence is unlikely to decline.
A nutritional biologist presented the idea that all the carbohydrates and fat in our food today dilute the protein our bodies need, driving us to eat more calories to make up for the discrepancy. An endocrinologist spoke of the scientific model behind the low-carb diet approach, suggesting eating patterns heavy in carbohydrates are uniquely fat promoting, while an evolutionary anthropologist argued many lean hunter-gatherer societies ate a lot of carbohydrates, with a special affinity for honey.
Others suggested the problem is ultraprocessed foods, the prepared and packaged goods that make up more than half of the calories Americans consume. A physiologist shared his randomized control trial showing people eat more calories and gain more weight on ultraprocessed diets compared with whole-food diets of the same nutrient composition. But it’s still unclear why these foods drive people to eat more, he said.
The mystery could be explained by the thousands of toxic substances ultraprocessed foods can carry in the form of fertilizers, insecticides, plastics and additives, argued one biochemist . Her research in cells has shown these chemicals interfere with metabolism.
Still others thought perhaps the problem is less about what we’re eating and more about what we’re not. An ethologist shared her work on the link between food insecurity and obesity in birds. When food becomes scarce, the animals eat fewer calories but gain more weight. Studies in humans have also found a “robust” association between food insecurity and obesity, she said — the so-called hunger obesity paradox.
To add to the complexity, the researchers made it clear that obesity can’t be thought of as one condition. They spoke of rare cases caused by single gene mutations or disorders; more commonly, obesity is believed to arise because of still murky gene-environment interactions. Perhaps they should have been talking about obesities the whole time.
By the end of the conference, the attendees were no closer to a unifying theory for the global rise in obesity — a condition that’s been with humans since at least Hippocrates but started to become widespread only after the debut of MTV. Yet in that short period, scientists, including many in the room, have learned a lot.
They’ve identified more than a thousand genes and variants that increase a person’s obesity risk. They’ve figured out that body fat is much more than a storage depot for energy and that not everyone with obesity goes on to develop its associated complications, which include cancer, Type 2 diabetes, high blood pressure, heart attack, stroke and premature death. They’ve made remarkable progress mapping out how the brain orchestrates feeding and adapts to different diets, altering food preferences along the way. But precisely what changed in recent history to affect these complex biological systems, the scientists couldn’t concur.
Since the meeting, I’ve been struck by the profound gap between the talks I heard and the weight conversation happening in our culture. No scientist spoke of any of the supposed fixes that fill diet books and store shelves, with the exception of the carbohydrate discussion. There wasn’t serious dialogue about cleanses, diet apps or intermittent fasting. No one suggested that supplements could help people lose weight or that metabolisms need boosting. The sole presenter on the gut microbiome argued that the human trials in obesity to date have mostly disappointed.
In other words, there were no quick fixes or magic hacks in that London meeting room. And while there was excitement about medicine’s incredible strides in treating patients with obesity , the effective drugs and surgeries weren’t talked about as end-all solutions for the public health crisis.
When I asked many of the researchers how they’d tackle obesity, given the uncertainties, they pointed to policies that would alter or regulate our environment, like outlawing junk food marketing to kids, banning vending machines in schools and making neighborhoods more walkable. They talked about changing the food system in ways that also address climate change — a related crisis once met with policy inertia that now has international momentum. But when it comes to obesity, governments are still accused of being nanny states if they try to intervene with regulation.
This is in part because instead of viewing obesity as a societal challenge, the individual choice bias dominates. It’s steeped with misunderstanding and blame, and it’s everywhere. People are simply told to eat more vegetables and exercise — the equivalent of tackling global warming by asking the public only to fly less or recycle. Diet gurus and companies mint billions off food and exercise fads that will ultimately fail.
When people can’t control their body weight, they often blame themselves. I recently interviewed a man who, after a brain tumor, developed severe obesity — a common side effect of his condition. The tumor went undiagnosed for months as doctors told him to diet and exercise more. But even today, he told me, the tumor just felt like “another excuse” for longtime weight struggles, so he doesn’t talk about it with anyone.
Others provide the shame, too. A recent Times of London column argued that fat shaming is a real solution to obesity, just as Bill Maher ranted earlier that the body positivity movement — a “joyful celebration of gluttony,” he said — harms people by condoning weight gain. Quite the contrary: Researchers have repeatedly found fat shaming promotes weight gain and harms. At least some of obesity’s negative health consequences are thought to be driven by stigma and discrimination, which results in poorer health care.
Until we see obesity as something that’s been imposed on societies, not as something individuals choose, the fat shaming, magic hacks and bad policies will continue. Until we stop blaming ourselves and one another and start focusing attention on environments and systems, the global obesity rate will continue its ascent — a trend no country has substantially reversed, not even in children.
Julia Belluz is a health journalist. She is writing a book about nutrition and metabolism.
The Times is committed to publishing a diversity of letters to the editor. We’d like to hear what you think about this or any of our articles. Here are some tips . And here’s our email: [email protected] .
Follow the New York Times Opinion section on Facebook , Twitter (@NYTopinion) and Instagram .
My Mother, Obesity and Me: Our Narrative. How Obesity Is Intimately Related to Biopsychosocial and Spiritual Factors
- Open Access
- First Online: 13 April 2022
Cite this chapter
You have full access to this open access chapter

- Eduardo Farías-Trujillo 4 , 5
Part of the book series: Public Health Ethics Analysis ((PHES,volume 7))
2918 Accesses
The word obesity invokes multiple connotations that contain a realm of disparate descriptions ranging from disease to disdain. There are few other human conditions that cause increased morbidity and mortality and affect millions of individuals worldwide yet is viewed by many as a character fault or moral failure. This paper explores the personal experience of obesity and how it is important to face obesity not only as a biological issue, but also a philosophical one, which has its roots in a complex phenomenon. This approach allows health professionals to propose a theoretical ethic about obesity, which goes beyond mere socio-economic-religious, and leads to an applied ethics built on the firm and solid foundations of knowledge diversity. The obese human being does not live in a world of simple events, but instead faces experiences – mystical, religious, artistic, linguistic – and, from there, configures their identity, builds personality and establishes interrelations and interdependencies. While recognizing the importance of strategies to reverse the trend of increasingly sedentary lifestyles, this paper points to the need for public health obesity reduction efforts to avoid stigmatizing people who cannot lose weight.
You have full access to this open access chapter, Download chapter PDF
Similar content being viewed by others

The Tipping of the Big Stone—And Life itself. Obesity, Moral Work and Responsive Selves Over Time

Biomassochism: Lacan and the ethics of weight cycling

Tipping the Scales of Truth: Why the Energy Balance Equation Is a Dangerous Lie
- Environmental influences
- Obesogenic environment
- Personal responsibility
Public Health Ethics Issue
World-wide, obesity is a growing health problem (Fox et al. 2019 , 1). The impact of this problem is clearly seen in Mexico. Over the past 20 years, obesity has increased steadily among Mexicans in conjunction with a transformation of the nutritional landscape. This transformation has involved increased availability of highly processed, inexpensive food; more advertising targeting fast food; and increased food consumption outside of the home. This has led to profound changes in the diet of a growing sector of Mexicans leading to increased consumption of food that contains high amounts of fat, sugar, and salt (Rivera et al. 2012 , 119–151).
Nutrition and foodbehaviors are often approached as a matter of personal responsibility. This creates a challenge for health officials who need to ensure there is a comprehensive approach to obesity that focuses on creating public policy for reducing food insecurity and malnutrition (Loring and Robertson 2014 ), promoting public health interventions that foster better eatinghabits, and avoiding approaches that blame or stigmatize individuals (Puhl and Heuer 2009 , 2010 ; Mexican Observatory of Non-communicable Diseases [OMENT] 2018 ).
Background Information
In Mexico, the Ministry of Health estimates that the total cost of obesity in 2017 was $12 billion and will continue to increase until reaching $13.6 billion by 2023, a projected increase of 13% over 6 years (Health Secretary of Mexico 2013 ). A study by the Mexican Institute of Competitiveness (IMCO) estimated that the total annual cost of diabetes associated with obesity amounted to $42 billion in 2013, of which 73% represented medical expenses, 15% work-related losses due to absenteeism, and 12% income losses due to premature mortality (IMCO 2015 ).
To address the growing costs associated with obesity, the Health Secretary of Mexico launched the National Strategy for Prevention and Control of Overweight, Obesity and Diabetes (Health Secretary of Mexico 2013 ). The government promoted this as an unprecedented effort to combat two of the main challenges to the health of Mexicans: overweight that affects seven out of 10 adults and three out of every 10 children, as well as diabetes that affects almost one in ten people. This strategy has three pillars: public health, medical care and health regulation/fiscal policy. For this strategy to be successful, it must consider that foodbehavior is not just a matter of individual willpower and personal responsibility determined by biological needs. Rather, food behavior is also impacted by social and cultural values, (Health Secretary of Mexico 2013 ). Focusing solely on diet and exercise will not solve the obesity problem.
The scientific community, as well as various international organizations (i.e., the World Health Organization, the Food and Agriculture Organization of the United Nations (FAO), the World Obesity Federation (WOF) and the World Cancer Research Fund (WCRF) have concluded that the global epidemic of overweight and obesity arises primarily from an environment that promotes obesity. (WHO 2018 , 2020 ; World Health Assembly 2004 ). Such an “obesogenic environment” (Swinburn et al. 2001 ) results from multimillion-dollar advertising for ultra-processed foods high in sugars, fat, and sodium, and the omnipresence and affordability of these products (World Health Assembly 2004 ).
On international and national scales, Mexico is an obese nation. According to the Organization for Economic Co-operation and Development (OECD), which comprises 35 countries worldwide, representing each continent, Mexico ranks as one of the nations with the highest adult obesity rate (OECD 2010 ). In schoolchildren without program food aid, the prevalence of obesity increased 97% between 2012 and 2018 (WHO 2018 ). In adolescents without program food aid, the prevalence of obesity increased 60% between 2012 and 2018. In adults with moderate food insecurity, obesity increased 10% between 2012 and 2018 (Shama-Levy et al. 2019 , 852).
In the face of such challenges, governments and society have not stood idly by. Massive campaigns that promote healthy eating habits, such as the consumption of fruits and vegetables, occur in almost all OECD countries. Mexico has the “5 fruits and vegetables a day” promotion, as well as regulations that seek to promote the consumption of fresh foods in season (5 x Día Verduras y Frutas, México 2006 ; Official Journal of the Federation [DOF] 2013 ). Likewise, social networks and mobile applications have encouraged users to reduce body weight and increase physical activity.
According to the National Institute of Public Health (INSP), Mexico is one of the countries with the highest incidence of obesity and diabetes (34% of the population in Mexico is obese and 9.2% have been diagnosed with diabetes) (INSP 2020 ). The health and economic implications are so large (Manzano 2017 ), that in 2016 the Health Ministry declared obesity and diabetes national public health emergencies (Rivera et al. 2018 ). Mexico is also a major consumer of sugary drinks, a known risk factor for obesity and diabetes. Up to 10% of all calories consumed by Mexican children and adults come from sugary drinks (National Health and Nutrition Survey [ENSANUT] 2018 ).
In January 2014, the Mexican government implemented a 10% tax to industrialized sugar sweetened beverages to curb the obesity and diabetes epidemic. Two years later, a first analysis by the National Institute of Public Health (NIPH) on the impact of this tax found that consumption of sugar sweetened beverages in the country had decreased by 6.1% (INSP 2020 ).
Obesity is not only a food problem; there are many factors that contribute to obesity, such as some genetic syndromes and endocrine disorders, (hypothyroidism, Cushing’s syndrome, tumors), medicines such as antipsychotics, antidepressants, antiepileptics, and antihyperglycemics, unhealthy lifestylehabits, age, unhealthy environments, family history and genetics, race or ethnicity and sex (Templeton 2014 ; Lee et al. 2019 ; Bolton and Gillett 2019 ). Educational and socioeconomic inequalities (Loring and Robertson 2014 ) also influence high rates of obesity. The obstacles and difficulties faced by many people in the labor market, such as lower recruitment, lower productivity and poor re-entry, reinforce these inequalities. In Mexico, as elsewhere, it is common to find that malnutrition and obesity coexist among the inhabitants of the same community and among the members of the same household (Pedraza 2009 , 108). This is because among lower socioeconomic groups, prenatal and infant nutrition is often inadequate because they receive less expensive fast or processed foods that are high in calories, fat, sugar, and salt, but poor in micronutrients (Headey and Alderman 2019 , 2020–2021).
Approach to the Narrative
In the following story, I share my personal story with obesity to illustrate the complex factors that impact weight and foodbehavior and how focusing on individual willpower and personal responsibility will not by itself solve the challenge of obesity.
My mother and I struggled with weight issues all our lives.
Since 1997, I have been a Catholic priest, but my priestly formation began back in 1982 at the tender age of 12. The teachings and practices of Catholicism, which emphasize individual responsibility and forgiveness, shaped my personality and approach to my and my mother’s obesity.
As my story will show, my mother could not recover from obesity because the social factors that sustain it are powerful. My mother had to face obesity due to her circumstances. My father was a worker in the United States; he had to be out of the country for half a year and my mother had to take care of the family. My father did not allow my mother to work outside of the home. So, sometimes we did not have enough money to buy food. Sometimes we had to rely upon family and friends for our meals. My parents’ relationship gradually deteriorated. However, my mother never wanted to permanently separate from my father. These marital conflicts and my mother’s tendency to worry about her children had an impact on her physical and mental health and ultimately her obesity.
My mother and I were always very close. My father’s absence because of his work, as well as the fact that I am the eldest of five siblings, led me to behave not only as her son, but as her confidant and support in the care of my brothers.
Although she was a strong, determined, tenacious woman, she could not and did not want to face her obesity. Although she wanted to have adequate weight and a good quality of life, she did not decide to fully cope with her obesity. It wasn’t just about weight; it was about a different way of living. She died with obesity, although not only because of it. On one occasion she went to my room and, with tears in her eyes, she asked me: “Am I never going to be healthy?” At that time, I believed strength of will was enough to face any physical, moral, or spiritual problem. So, I answered to her: “It is enough that you decide to do it”. I was wrong. There is no universal recipe for recovering from obesity.
In 2011, I joined a support group to address my obesity. Thanks to the internal dynamics of this group I became aware of how my physical and emotional health impacted my weight. I lost 46 pounds in 1 year. I discovered that addressing my obesity was not a matter of willpower, but of goodwill, because it is not about following crash diets or extreme exercises, but about adopting a permanent healthy lifestyle.
My father, who is now 72 years old, has been an athlete and an amateur boxer all his life. To this day he is a strong and vigorous man who takes care of his physical health. He was always trying to get me to exercise, to train, to run, to jump rope. When the movie, Rocky , appeared in Mexico, 2 years after it appeared in the United States, my father took me to see it. As I watched the movie, I saw my father: an athletic, handsome sportsman who took care of his body and exhorted me to imitate him. My father wanted me to be like him or like my cousins, who possessed different physical skills than me. He told me that I had to be like them—that they ran, climbed trees and were not fat like me.
In 1982, when I was 12 years old, I participated in track and field at school. My team, the Blues, lacked competitors for a 2.5-mile race. I had never run that distance and, when the coach asked me to run this race, my first reaction was to refuse. Two and a half miles are 12 and a half laps around a soccer field. After 28 min and 30 s, I finished in last place, but I earned points for my team. This experience brought about a fundamental change in my life. I realized that I had many physical abilities that were not the same as my dad’s; they were also not the same abilities as other boys’ my age. My abilities were different, but real. When the time came for the awards, some of my classmates told me, “We didn’t know you were capable of this.” I had pain in my body, but joy in my heart. When I got home, I shared with my family what I had achieved. My brothers, sisters and my parents congratulated me, when I told them that this moment had been like an epiphany, a revelation. I started participating in other sports, because, unlike my father, I was not interested in in boxing. I discovered that I had ability for tennis, Tae Kwon Do, swimming, soccer, hiking, and jogging. At first, engaging in sports, caring for myself, my appearance and health, were influenced by family and social pressures. Afterwards, having a good quality of life was an issue I internalized and made mine. I learned to lead a new way of life.
I entered the Diocesan Seminary in 1985. An eleven-year stage for priestly ordination began. I was 15 years old, 5 feet, 7 inches tall, weighed 172 pounds, and my pants size was 32. My participation in sports and the intensity of my studies resulted in me losing weight and I dropped to size 28. In December 1985, when I went back home to see my father, whom I had not seen since June because of his work in United States, I thought he would be proud of my great achievement. I had lost weight, I was on the Tae Kwon Do team, I was part of the soccer team, and I was running or walking almost every day. When he saw me, my father said: “You are very skinny.” I wondered where the congratulations were, the recognition, the applause, the hug. I had thought that when my father saw that I had lost weight, he would be happy, he would feel proud of me and congratulate me. Within me, I experienced a kind of male rivalry between father and son because of my weight and physical appearance. When he said “you are very skinny” it broke my heart. Instead of a hug and a congratulation, I felt that he saw me as a rival and that his message was: “I am better than you.” I thought he should know that I was following his example and that he should feel happy.
In the Seminary I received many awards for my academic achievements. I obtained an average of A+ during the 11 years of priestly formation. As a prize for my intellectual capacity and my responsibility, I obtained the opportunity to study in Rome. While in Rome, I swam, ran, and went to the gym. I also was careful about my diet, so I returned from Rome weighing 165 pounds. However, I was not able to maintain this healthy lifestyle when I returned from Rome.
I came back to Mexico and the bishop appointed me director of a preparatory school. These were years of intense academic work, including contact with students, parents, staff, and administration. In addition, I provided marital counseling. I worked all day long and into the evening. The daily stresses contributed to my putting on weight. I became an obese person.
I tried to exercise. I played soccer and ran, but I could not manage a healthy lifestyle. When the evening meetings were prolonged, the dinners were plentiful, and since I skipped meals during the day, I overate at dinner. These attitudes created a vicious cycle. Not eating during the day led to overindulgence at night. To compensate, the next day I would forego breakfast or lunch and just drink coffee.
While I knew that many factors impacted my obesity, including my biology, and social and emotional factors, I was still focused on personal responsibility. I felt that I, like everyone else, had to take personal responsibility for starting a recovery process. I hit rock bottom when I realized that my obesity was preventing me from having a good quality of life.
At the time I went to Rome, my mother, weighed 221 pounds, but she was 5 feet, 3 inches tall. Although obesity is not just a matter of weight, she and I realized what was happening with us. Eating more food than we needed made us tired, and our growing immobility saddened us. Things did not get better and our health became precarious. In a span of just 2 years my weight ballooned from 165 pounds to 203 pounds. What was going on inside manifested itself on the outside. I once heard someone say that the body screams what silences the soul.
A friend of mine started losing weight and I asked him how he was doing it, to which he replied that he was receiving treatment from a nutritionist and that it really worked. Although it took me a few months; I finally went to see the nutritionist. The nutritionist told me that a healthy lifestyle includes regular exercise, a balanced relationship with food, enough sleep and rest time, and not forgetting good social relationships. If I had obesity problems it was because I had stopped having a healthy lifestyle (i.e., I was not taking care of my body, my mind or my relationships). The nutritionist became an important teacher for me, because he proposed a diet of specific foods, appropriate portions, fixed schedules for eating, exercise and establishing good social relationships. I knew that I needed a new way of life that included working to improve and maintain the health of my body; to respect, enjoy, and love my body as if it was a part of me and not my enemy.
What happened next was that I came home and talked to my mother and told her we should start together with this new lifestyle. I knew that I theory without practice is just information, because it was not just about improving our body image, but about improving our personal confidence, our psychological state and our functioning in the different areas of our lives. We had to assimilate that love for the body does not lead to creating a perfect body, but it is a condition of possibility to be happy in an imperfect, fragile body, full of challenges.
I started following the diet suggested by the nutritionist. I was walking an hour a day. In 3 weeks, I lost 13 pounds. I lost 46 pounds in a year. Deep down I was proud, because I had “willpower” and, under this premise, I asked my mother to do the same, to start this new lifestyle with me, that she should be strong, that she should eat only what was necessary and that she would soon reach good weight, but she did not, because even though she was a strong woman, determined and courageous, from my point of view, was weak in the face of obesity.
I confess I didn’t consider her genetic predisposition and environmental triggers conspired against her. I did not know that in the face of these conditions, little can be done by just focusing on individual factors. My mother suffered from hypothyroidism and was 23 years older than me. Although I took this into account, my focus still was on my mother’s willpower. My father, my brothers and I often blamed her for her excessive weight. We failed to understand all the pressures and circumstances that influenced her obesity. My mother had to choose the food, she had to adjust to a budget, she had to consider the different preferences of six different people and she had to cook something that everyone liked.
My main mistake was that I thought my mother should be like me, i.e., that it was enough for her to decide to change the way she ate, because I had done it that way. I wanted to lose weight because my motivation was health. I thought that everyone would react like me, that is, they would want to have a “normal” weight for health reasons. I didn’t consider that each person has different motivations not only to provide food to others, but also to eat.
What did my struggle with obesity teach me? It taught me that a complex of factors that range from the individual and physiological to the social contribute to the outcome of body weight. Obesity is about biopsychosocial and spiritual factors. That is why an integrated approach makes sense and is most effective. The whole community must get involved in a sustained way and engage on all levels from individual behavior, nutrition, and physical activity up to the individual’s environment, broadly conceived. The immediate social environment, the family, plays a key role in prevention by establishing healthy attitudes. Attitudes and good habits formed in the family in one generation pass on to children and can have a multigenerational effect on health. The family is a good place to start, but efforts cannot end there. Governments also play a role. Interventions that restructure the environment to make healthier choices easier and make healthy foods more available and cheaper play an important role in tackling obesity.
A holisticapproach will impact the entire population down to the level of individual behaviors. The focus should be on health as the motivator and the desired outcome rather than fixating on weight. This fixation goes hand in hand with stigmatizing the person, rather than focusing on the problem and the behaviors. I know. Fixating on some ideal body type and weight I was never destined to realize was my pathway to stigmatizing myself, one that thank God I eventually learned to avoid.
Questions for Discussion
Are stories of personal struggles with obesity useful? If so, what makes them useful; if not, why not?
Some people think stigmatizing obese individuals or making them feel guilty about their condition can help them. Do you agree with this idea? Why or why not?
Public health professionals emphasize that obesity is a disease. What do you see as the advantages and disadvantages of this view?
Obesogenic environments play a role in the obesity epidemic. How great a role do you think environments play, especially compared to individual behavior?
Do you think it possible to address the obesity epidemic without in some way limiting or restricting peoples’ lifestyle choices or access to obesogenic foods?
The narrative suggests that individual behavior, family life, and obesogenic environments all play a role in the obesity epidemic.
Do you agree that a holisticapproach is necessary or the best strategy to address the problem? Why or why not?
Do you think that focusing on the family, an obesogenic environment, and the idea of obesity as a disease run the risk of giving obese individuals an excuse not to take responsibility for their condition? If so, how would you address this concern?
What conditions do you think most influence the obesity epidemic and why?
5 x DÍA VERDURAS Y FRUTAS, MÉXICO. 2006. Revista Chilena de Nutricion 33 (S1): S316–S317. https://doi.org/10.4067/S0717-75182006000300016 .
Article Google Scholar
Bolton, Derek, and Grant Gillett. 2019. The Biopsychosocial Model of Health and Disease: New Philosophical and Scientific Developments . Cham: Palgrave Pivot. https://link.springer.com/content/pdf/10.1007/978-3-030-11899-0.pdf .
Book Google Scholar
Fox, Ashley, Wenhui Feng, and Victor Asal. 2019. What Is Driving Global Obesity Trends? Globalization or “Modernization”? Globalization and Health 15 (32). https://doi.org/10.1186/s12992-019-0457-y .
Headey, Derek D., and Harold H. Alderman. 2019. The Relative Caloric Prices of Healthy and Unhealthy Foods Differ Systematically Across Income Levels and Continents. The Journal of Nutrition 149 (11): 2020–2033. https://doi.org/10.1093/jn/nxz158 .
Health Secretary of Mexico. 2013. National Strategy for the Prevention and Control of Overweight, Obesity and Diabetes . First edition, September. https://www.gob.mx/cms/uploads/attachment/file/276108/estrategia_sobrepeso_diabetes_obesidad.pdf .
Lee Alexandra, Michelle Cardel, and William T. Danahoo. 2019. “Social and Environmental Factors Influencing Obesity.” In ENDOTEXT, ed. K.R. Feingold, B. Anawalt, A. Boyce, et al. South Dartmouth: MDText.com. https://www.ncbi.nlm.nih.gov/books/NBK278977/ .
Google Scholar
Loring, Belinda, and Aileen Robertson. 2014. Obesity and Inequities. Guidance for Addressing Inequities in Overweight and Obesity . Copenhagen: WHO Regional Office for Europe. http://www.euro.who.int/__data/assets/pdf_file/0003/247638/obesity-090514.pdf?ua=1 .
Manzano, Elena Analuisa. 2017. Relación del Sobrepeso y Obesidad con el Rendimiento Laboral en Trabajadores de una Empresa Metalmecánica en México. Revista Colombiana de Salud Ocupacional 6 (4): 5–10. https://revistas.unilibre.edu.co/index.php/rc_salud_ocupa/article/view/4940 .
Mexican Institute of Competitiveness (IMCO). 2015. La Corrupción en México: Transamos y no Avanzamos . https://periodicooficial.jalisco.gob.mx/content/la-corrupcion-en-mexico-transamos-y-no-avanzamos .
Mexican Observatory of Non-communicable Diseases (OMENT). 2018. Epidemiological Overview: Non-communicable Diseases . Secretary of Health, Mexico. https://epidemiologia.salud.gob.mx/gobmx/salud/documentos/pano-OMENT/panoepid_ENT2018.pdf .
National Health and Nutrition Survey 2018 (ENSANUT 2018). 2018. https://ensanut.insp.mx/encuestas/ensanut2018/doctos/informes/ensanut_2018_presentacion_resultados.pdf .
National Institute of Public Health (INSP). 2020. Tax to Sugar Sweetened Beverages in Mexico is Expected to Reduce Obesity and Diabetes . https://www.insp.mx/epppo/blog/4446-sweetened-beverages-mexico.html .
Official Journal of the Federation (DOF). 2013. Official Mexican STANDARD NOM-043-SSA2-2012, Basic Health Services . Promotion and Education for Health in Alimentary Matters. Criteria for Providing Guidance. http://dof.gob.mx/nota_detalle.php?codigo=5285372&fecha=22/01/2013 .
Organization for Economic Co-operation and Development (OECD). 2010. Obesity and the Economics of Prevention: Fit Not Fat . Paris: OECD Publishing. https://doi.org/10.1787/9789264084865-en .
Pedraza, Dixis Figueroa. 2009. Obesity and Poverty: Conceptual References for Its Analysis in Latin America. Saúde e Sociedade 18 (1): 103–117. http://www.scielo.br/pdf/sausoc/v18n1/11.pdf .
Puhl, Rebecca M., and Chelsea A. Heuer. 2009. The Stigma of Obesity: A Review and Update. Obesity 17 (5): 941–964. https://doi.org/10.1038/oby.2008.636 .
———. 2010. Obesity Stigma: Important Considerations for Public Health. American Journal of Public Health 100 (6): 1019–1028. https://doi.org/10.2105/AJPH.2009.159491 .
Rivera Dommarco, Juan Ángel, Mauricio Hernández Ávila, Carlos A. Aguilar Salinas, Felipe Vadillo Ortega, and Ciro Murayama Rendon. 2012. Obesidad en México: Recomendaciones para una Política de Estado . México: UNAM. https://www.anmm.org.mx/publicaciones/Obesidad/obesidad.pdf .
Rivera Dommarco, Juan Ángel, Mónica Arantxa Colchero Aragonés, Mario Luis Fuentes, Teresita González de Cosío Martínez, Carlos A. Aguilar Salinas, Gonzalo Hernández Licona, and Simón Barquera. 2018. La Obesidad en México. Estado de la Política Pública y Recomendaciones para su Prevención y Control . México: Instituto Nacional de Salud Pública. https://www.insp.mx/produccion-editorial/novedades-editoriales/4971-obesidad-mexico-politica-publica-prevencion-control.html .
Shama-Levy, T., Ismael Campos-Nonato, Lucía Cuevas-Nasu, Lucía Hernández-Barrera, María Del Carmen, Juan Rivera-Dommarco Morales-Ruán, and Simón Barquera. 2019. Overweight and Obesity in Mexican Vulnerable Population. Results of Ensanut 100k. Salud Pública de México 61 (6): 852–865. https://www.medigraphic.com/cgi-bin/new/resumenI.cgi?IDARTICULO=90731 .
Swinburn, Boyd, Gary Sacks, Kevin D. Hall, Klim McPherson, Diane T. Finegood, Marjory L. Moodie, and Steven L. Gortmaker. 2001. The Global Obesity Pandemic: Shaped by Global Drivers and Local Environments. The Lancet 378 (9793): 804–814.
Templeton, Arnoud J. 2014. Obesity and Women’s Health. Facts, Views and Vision in Obstetrics, Gynaecology, and Reproductive Health 6 (4): 175–176. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4286855/ .
World Health Assembly. 2004. Fifty-Seventh World Health Assembly, Geneva, 17–22 May 2004: Summary Records of Committees, Reports of Committees . World Health Organization. https://apps.who.int/iris/handle/10665/260147 .
World Health Organization. 2018. Obesity and Overweight . https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight .
———. 2020. The WHO Child Growth Standards . https://www.who.int/childgrowth/standards/en/ .
Download references
Author information
Authors and affiliations.
Clarkson University, Potsdam, NY, USA
Eduardo Farías-Trujillo
Bioethics Unit, Faculty of Philosophy, Autonomous University of Queretaro, Queretaro, Mexico
You can also search for this author in PubMed Google Scholar
Corresponding author
Correspondence to Eduardo Farías-Trujillo .
Editor information
Editors and affiliations.
Centers for Disease Control and Prevention, Atlanta, GA, USA
Drue H. Barrett & Leonard W. Ortmann &
Bioethics Fellow, Cleveland, OH, USA
Stephanie A. Larson
Additional information
Disclaimer: This paper is presented for instructional purposes only. The ideas and opinions expressed are the author’s own. The paper is not meant to reflect the official position, views, or policies of the editors, the editors’ host institutions or the author’s host institution.
Rights and permissions
Open Access This chapter is licensed under the terms of the Creative Commons Attribution 4.0 International License ( http://creativecommons.org/licenses/by/4.0/ ), which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license and indicate if changes were made.
The images or other third party material in this chapter are included in the chapter’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the chapter’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder.
Reprints and permissions
Copyright information
© 2022 The Author(s)
About this chapter
Farías-Trujillo, E. (2022). My Mother, Obesity and Me: Our Narrative. How Obesity Is Intimately Related to Biopsychosocial and Spiritual Factors. In: Barrett, D.H., Ortmann, L.W., Larson, S.A. (eds) Narrative Ethics in Public Health: The Value of Stories. Public Health Ethics Analysis, vol 7. Springer, Cham. https://doi.org/10.1007/978-3-030-92080-7_15
Download citation
DOI : https://doi.org/10.1007/978-3-030-92080-7_15
Published : 13 April 2022
Publisher Name : Springer, Cham
Print ISBN : 978-3-030-91443-1
Online ISBN : 978-3-030-92080-7
eBook Packages : Religion and Philosophy Philosophy and Religion (R0)
Share this chapter
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Publish with us
Policies and ethics
- Find a journal
- Track your research
Home — Essay Samples — Nursing & Health — Obesity — Essay On Obesity In America
Essay on Obesity in America
- Categories: Obesity
About this sample

Words: 991 |
Published: Mar 5, 2024
Words: 991 | Pages: 2 | 5 min read

Cite this Essay
Let us write you an essay from scratch
- 450+ experts on 30 subjects ready to help
- Custom essay delivered in as few as 3 hours
Get high-quality help

Verified writer
- Expert in: Nursing & Health

+ 120 experts online
By clicking “Check Writers’ Offers”, you agree to our terms of service and privacy policy . We’ll occasionally send you promo and account related email
No need to pay just yet!
Related Essays
1 pages / 476 words
1 pages / 619 words
3 pages / 1382 words
2 pages / 866 words
Remember! This is just a sample.
You can get your custom paper by one of our expert writers.
121 writers online
Still can’t find what you need?
Browse our vast selection of original essay samples, each expertly formatted and styled
Related Essays on Obesity
According to recent studies, obesity has become a global epidemic, affecting millions of people worldwide. Obesity is not only a personal health issue but also a societal concern. It is linked to various health problems and has [...]
Obesity has become a major health issue in recent times, with over 39% of adults around the world being overweight and 13% being obese. In the United States, 42.4% of adults are obese, costing the country a staggering $147 [...]
In recent years, the issue of obesity has become a global epidemic. Obesity is a condition where a person has an excessive amount of fat, which can lead to numerous health problems. According to the World Health Organization [...]
According to the World Health Organization, in 2016, more than 1.9 billion adults were overweight, of which around 650 million were obese. In the United States alone, more than 42% of the population is considered obese. This [...]
“What if a war on obesity only makes the problem worse”? argues Author Daniel Engber in his article “Glutton Intolerance”. Discrimination against the obese in our society makes the obesity problem worse. The treatment against [...]
Throughout recent years obesity has been a very important topic in our society. It has continued to rise at high rates especially among children. This causes us to ask what are the causes of childhood obesity? There are many [...]
Related Topics
By clicking “Send”, you agree to our Terms of service and Privacy statement . We will occasionally send you account related emails.
Where do you want us to send this sample?
By clicking “Continue”, you agree to our terms of service and privacy policy.
Be careful. This essay is not unique
This essay was donated by a student and is likely to have been used and submitted before
Download this Sample
Free samples may contain mistakes and not unique parts
Sorry, we could not paraphrase this essay. Our professional writers can rewrite it and get you a unique paper.
Please check your inbox.
We can write you a custom essay that will follow your exact instructions and meet the deadlines. Let's fix your grades together!
Get Your Personalized Essay in 3 Hours or Less!
We use cookies to personalyze your web-site experience. By continuing we’ll assume you board with our cookie policy .
- Instructions Followed To The Letter
- Deadlines Met At Every Stage
- Unique And Plagiarism Free
IMAGES
VIDEO
COMMENTS
Obesity is a personal health care responsibility. This vested responsibility implies that individuals should participate proactively and beyond a reasonable doubt in safeguarding healthy living. Obesity complications are associated with the choice of food eaten, and the shaped body takes as a result. The consumers should remain protected as ...
Without considering aspects of responsibility, obesity management is severely compromised. There are at least two sides to personal responsibility: medicalizing obesity, which reduces it, and parental supervision, which emphasizes it, since fat children are at high risk for adult obesity ( 7 ). Finally, I suggest an integrated nine-level ...
In Study 2, 125 US adults read one of three randomly assigned online passages attributing obesity to personal responsibility, biology, or the 'food environment.' All participants in both studies ...
The concept of personal responsibility has been central to social, legal, and political approaches to obesity. It evokes language of blame, weakness, and vice and is a leading basis for inadequate ...
It found that 72 to 98 percent of obesity-related media reports emphasize personal responsibility for weight, compared with 40 percent of scientific papers. A recent study by Drexel University researchers also quantified the political polarization around public health measures.
problem, often seeing obesity as a cosmetic issue most appropriately addressed by personal responsibility. The re-ality is that most, if not all, of these perspectives will need to change if the growth and consequences of the epidemic in the years to come is to be arrested. Over the past several decades, psychologists have made
The obesity pandemic has resulted in millions of deaths and untold suffering. And if you're not mad yet, brace yourself for my next video, The Role of Corporate Influence in the Obesity Epidemic. This is the ninth in this 11-part series. If you missed any, see: The Role of Diet vs. Exercise in the Obesity Epidemic.
The view that obesity is a matter of personal responsibility is the prevailing message in the media. 29-31,40,41 News coverage of the personal causes and solutions to obesity significantly outnumber other societal attributions of responsibility. 29 Entertainment media also communicate anti-fat messages and reinforce perceptions that body ...
In this essay, I take a closer look at what personal responsibility means in connection to the "problem" of obesity and recommended solutions. 2 What we find in obesity discourse is that the language of personal responsibility sometimes has a moral dimension to it; although the attribution of moral responsibility rarely comes equipped with any clear criteria of application.
In this article, we will thus argue that in the context of dysregulation of hunger and satiety contributing to the obesity epidemic, a wider discourse related to personal responsibility and the stigma of obesity is needed to enhance understanding, prevention, and treatment of this complex disease. Obesity is a chronic disease requiring ...
Obesity has become a global epidemic and is one of today's most public health problems worldwide. Obesity poses a major risk for a variety of serious diseases including diabetes mellitus, non-alcoholic liver disease (NAFLD), cardiovascular disease, hypertension and stroke, and certain forms of cancer (Bluher, 2019).Obesity is mainly caused by imbalanced energy intake and expenditure due to a ...
Guest Essay. Scientists Don't Agree on What Causes Obesity, but They Know What Doesn't. Nov. 21, 2022. ... As long as we treat obesity as a personal responsibility issue, its prevalence is ...
In Mexico, the Ministry of Health estimates that the total cost of obesity in 2017 was $12 billion and will continue to increase until reaching $13.6 billion by 2023, a projected increase of 13% over 6 years (Health Secretary of Mexico2013).A study by the Mexican Institute of Competitiveness (IMCO) estimated that the total annual cost of diabetes associated with obesity amounted to $42 billion ...
The aim of this article is to review literature data about personal and social responsibility in relation to obesity. Discover the world's research 25+ million members
The obesity epidemic is not just a matter of personal responsibility or willpower, but is influenced by a complex interplay of social, economic, and environmental factors. In this essay, we will explore the causes and consequences of obesity in America, as well as potential solutions to address this pressing issue.
Obesity rates have nearly tripled since 1975. As of 2016, more than 2.1 billion people worldwide are overweight or obese. We live in a blame culture, where everyone is quick to point fingers at all others before looking at their own actions and taking personal responsibility for their health. The stance on obesity is no different.
The government's continued emphasis on personal responsibility, coupled with a national sympathy towards, and fervent desire to support and protect, the NHS, risks further shaming marginalised people who are living with obesity and who are unable to assume personal responsibility for their excess weight because of their inability to choose ...
Obesity And Personal Responsibility. Satisfactory Essays. 213 Words. 1 Page. Open Document. According to American Journal of Clinical Nutrition, the poor tend toward greater obesity because eating energy-dense, highly palatable, refined foods is cheaper per calorie consumed than buying fish and fresh fruits and vegetables. One explanation for ...
Personal Responsibility And Obesity Essay. Good Essays. 1823 Words. 8 Pages. 8 Works Cited. Open Document. In the United States, there are many people who believe that if it wasn't for fast food restaurants, they would be eating healthier and wouldn't be overweight. People have even tried to sue fast food restaurants for their own self ...
Open Document. There are many people who believe that obesity is a matter of personal responsibility. Many people think it is Americans are the ones who to blame and not the fast food industry. Many people may say that it is easy to blame obesity on what Americans eat. However, these people do not realize that many Americans cannot afford ...
Personal Responsibility And Obesity Essay. Personal Responsibility and Obesity. Jim Rohn once said, "You must take personal responsibility. You cannot change the circumstances, the seasons, or the wind, but you can change yourself. That is something you have charge of.". In our busy lifestyles, it becomes easy to lose track of what is ...