Learn how UpToDate can help you.
Select the option that best describes you
- Medical Professional
- Resident, Fellow, or Student
- Hospital or Institution
- Group Practice
- Patient or Caregiver
- Find in topic

RELATED TOPICS
INTRODUCTION
Diagnosis and management of face and brow presentations will be reviewed here. Other cephalic malpresentations are discussed separately. (See "Occiput posterior position" and "Occiput transverse position" .)
Prevalence — Face and brow presentation are uncommon. Their prevalences compared with other types of malpresentations are shown below [ 1-9 ]:
● Occiput posterior – 1/19 deliveries
● Breech – 1/33 deliveries
7.10 Brow presentation
Brow presentation constitutes an absolute foeto-pelvic disproportion, and vaginal delivery is impossible (except with preterm birth or extremely low birth weight).
This is an obstetric emergency, because labour is obstructed and there is a risk of uterine rupture and foetal distress.
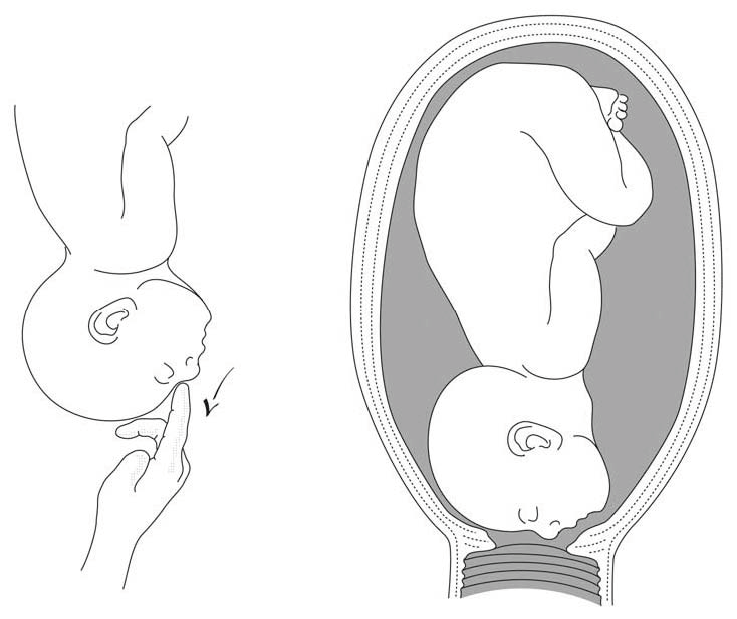
7.10.1 Diagnosis
- Head is high; as with a face presentation, there is a cleft between the head and back, but it is less marked.
- the chin (it is not a face presentation),
- the posterior fontanelle (it is not a vertex presentation).
Figures 7.9 - Brow presentation

Any mobile presenting part can subsequently flex. The diagnosis of brow presentation is, therefore, not made until after the membranes have ruptured and the head has begun to engage in a fixed presentation. Some brow presentations will spontaneously convert to a vertex or, more rarely, a face presentation.
During delivery, the presenting part is slow to descend: the brow is becoming impacted.
7.10.2 Management
Foetus alive.
- Perform a caesarean section. When performing the caesarean section, an assistant must be ready to free the head by pushing it upward with a hand in the vagina.
- Convert the brow presentation to a face presentation: between contractions, insert the fingers through the cervix and move the head, encouraging extension (Figures 7.10).
- Attempt internal podalic version ( Section 7.9 ).
Both these manoeuvres pose a significant risk of uterine rupture. Vacuum extraction, forceps and symphysiotomy are contra-indicated.
Foetus dead
Perform an embryotomy if the cervix is sufficiently dilated (Chapter 9, Section 9.7 ) otherwise, a caesarean section.
Planning for a baby?
- Preconception Health
- Preparing for Pregnancy
- Assisted Pregnancy
- Second Pregnancy
Already Pregnant?
- Pregnancy Week by Week
- Health & Safety
- Live life better
- Preparing for the baby
- Pregnancy Diet & Fitness
Have a Baby?
- Baby Milestones
- Baby Basics
- Mother Care
- Activity & Fun
Have a Toddler?
- Toddler Mile Stones
- Toddler Basics
- Food & Feeding
- Child Safety & Health
- Games & Playtime
- Special Child
Positive Parenting
- Health & Hyginie
- Learning and Development
- Family Basics
Child Safety
- Special child Care
- Planning for Future
- Play, Games, activity & Fun
Life Skills
Premature baby, baby products, health & safety, what is brow presentation what are its complications.
Written by Editorial Team
Editorial Team
With a rich experience in pregnancy and parenting, our team of experts create insightful, well-curated, and easy-to-read content for our to-be-parents and parents at all stages of parenting..
What Is Brow Presentation?
What leads to brow presentation, diagnosis of brow presentation, how to avoid c-section if baby is in brow presentation, what complications can arise due to brow presentation.

- Polyhydramnios : Excess amniotic fluid can make it difficult for the baby’s head to take a flexed position
- Size and shape of the pelvis: Abnormally shaped and sized pelvis can make it difficult for the baby to pick up a vertex presentation. Android pelvis, which has a triangular or heart-shaped inlet with a narrower front part, is usually behind most of the brow presentations. Similarly, contracted pelvis, a pelvis that is abnormally small, can cause brow presentation
- Fetal abnormality: Fetal abnormalities such as hydrocephalus, anencephaly and neck masses accounts for the majority of brow presentations
- Premature birth/low birth weight baby: If the baby is born prematurely or if the baby is having low birth weight , the chances of brow presentation increases
- Big baby : If the baby is larger than normal size, the baby tends to extend its head instead of curling inward
- Multiple pregnancies: Multiple pregnancies also increase the risk of brow presentation
- Multiple nuchal cords: If the umbilical cord wraps around the baby’s neck, obviously, it cannot tuck its chin into the chest. In such cases, the baby tends to be brow or face presentations
- Laxity of the uterus: If the uterine wall loses its firmness, the baby may not able to hold its chin tucked to the chest firmly and the baby tends to be in brow presentation
- Cephalopelvic disproportion (CPD): If the mother’s pelvis and the baby’s head are not proportionate to each other, brow presentation can happen

- Manual rotation: Doctor inserts his hand through the cervix and tries to flex the baby’s head
- The baby’s head should be engaged in the pelvis and should be in a front anterior position
- The pelvis should have sufficient room to permit the ventouse cup to be inserted posteriorly and to reach the occiput
- Ability and experience of the obstetrician
- How favorable is the position of the baby’s head inside the pelvis
- Available space inside the pelvis
- Increased chances of spinal cord injury are associated with brow presentation
- Fetal distress
- Abnormal shape of the baby’s head after delivery
- Prolonged labor
- Increased chances of using forceps which in turn increases the chances of facial trauma
- Obstructed labor
Advantages Of Saffron During Pregnancy
Saffron is the dried stigma of Crocus Sativus flower, i.e. the thread-like part at the centre which contains pollen.
Editorial Team,
With a rich experience in pregnancy and parenting, our team of experts create insightful, well-curated, and easy-to-read content for our to-be-parents and parents at all stages of parenting. Read more.

Responses (0)
Want curated content sharply tailored for your exact stage of parenting, read this next, related articles.

Strawberry During Pregnancy – Why Should This Fruit Be on Your Pregnancy Platter?

Viable v/s Non-Viable Pregnancy – What are They and Top Causes

Eno During Pregnancy – Is it Safe to Consume and Best Alternatives

Meditation During Pregnancy

Sodium Citrate During Pregnancy – Is It Safe to Take?
Glucon D During Pregnancy- Is it Safe to Drink and Benefits
Sponsored content
Discover great local businesses around you for your kids..
Get regular updates, great recommendations and other right stuff at the right time.
Premium Access
Join our community of 50K+ Moms and get access to exclusive features & resources in our app.
Pay Rs 25/- and read this article (One time access)

Our site uses cookies to make your experience on this site even better. We hope you think that is sweet.
Create account
Focus your wanderlust. create your account to get curated stories and recommendations., already have an account sign in.
Don't have an account? Sign up forgot password?
Get curated personalized content., articles and resources served personalized as per the stage of your parenting., already have an account login, choose one..

Enter dates
- Physician Physician Board Reviews Physician Associate Board Reviews CME Lifetime CME Free CME
- Student USMLE Step 1 USMLE Step 2 USMLE Step 3 COMLEX Level 1 COMLEX Level 2 COMLEX Level 3 96 Medical School Exams Student Resource Center NCLEX - RN NCLEX - LPN/LVN/PN 24 Nursing Exams
- Nurse Practitioner APRN/NP Board Reviews CNS Certification Reviews CE - Nurse Practitioner FREE CE
- Nurse RN Certification Reviews CE - Nurse FREE CE
- Pharmacist Pharmacy Board Exam Prep CE - Pharmacist
- Allied Allied Health Exam Prep Dentist Exams CE - Social Worker CE - Dentist
- Point of Care
- Free CME/CE
Delivery, Face and Brow Presentation
Introduction.
The term presentation describes the leading part of the fetus or the anatomical structure closest to the maternal pelvic inlet during labor. The presentation can roughly be divided into the following classifications: cephalic, breech, shoulder, and compound. Cephalic presentation is the most common and can be further subclassified as vertex, sinciput, brow, face, and chin. The most common presentation in term labor is the vertex, where the fetal neck is flexed to the chin, minimizing the head circumference.
Face presentation – an abnormal form of cephalic presentation where the presenting part is mentum. This typically occurs because of hyperextension of the neck and the occiput touching the fetal back. Incidence of face presentation is rare, accounting for approximately 1 in 600 of all presentations. [1] [2] [3]
In brow presentation, the neck is not extended as much as in face presentation, and the leading part is the area between the anterior fontanelle and the orbital ridges. Brow presentation is considered the rarest of all malpresentation with a prevalence of 1 in 500 to 1 in 4000 deliveries. [3]
Both face and brow presentations occur due to extension of the fetal neck instead of flexion; therefore, conditions that would lead to hyperextension or prevent flexion of the fetal neck can all contribute to face or brow presentation. These risk factors may be related to either the mother or the fetus. Maternal risk factors are preterm delivery, contracted maternal pelvis, platypelloid pelvis, multiparity, previous cesarean section, black race. Fetal risk factors include anencephaly, multiple loops of cord around the neck, masses of the neck, macrosomia, polyhydramnios. [2] [4] [5]
These malpresentations are usually diagnosed during the second stage of labor when performing a digital examination. It is possible to palpate orbital ridges, nose, malar eminences, mentum, mouth, gums, and chin in face presentation. Based on the position of the chin, face presentation can be further divided into mentum anterior, posterior, or transverse. In brow presentation, anterior fontanelle and face can be palpated except for the mouth and the chin. Brow presentation can then be further described based on the position of the anterior fontanelle as frontal anterior, posterior, or transverse.
Diagnosing the exact presentation can be challenging, and face presentation may be misdiagnosed as frank breech. To avoid any confusion, a bedside ultrasound scan can be performed. [6] The ultrasound imaging can show a reduced angle between the occiput and the spine or, the chin is separated from the chest. However, ultrasound does not provide much predicting value in the outcome of the labor. [7]
Anatomy and Physiology
Register for free and read the full article, learn more about a subscription to statpearls point-of-care.
Before discussing the mechanism of labor in the face or brow presentation, it is crucial to highlight some anatomical landmarks and their measurements.
Planes and Diameters of the Pelvis
The three most important planes in the female pelvis are the pelvic inlet, mid pelvis, and pelvic outlet.
Four diameters can describe the pelvic inlet: anteroposterior, transverse, and two obliques. Furthermore, based on the different landmarks on the pelvic inlet, there are three different anteroposterior diameters, named conjugates: true conjugate, obstetrical conjugate, and diagonal conjugate. Only the latter can be measured directly during the obstetric examination. The shortest of these three diameters is obstetrical conjugate, which measures approximately 10.5 cm and is a distance between the sacral promontory and 1 cm below the upper border of the symphysis pubis. This measurement is clinically significant as the fetal head must pass through this diameter during the engagement phase. The transverse diameter measures about 13.5cm and is the widest distance between the innominate line on both sides.
The shortest distance in the mid pelvis is the interspinous diameter and usually is only about 10 cm.
Fetal Skull Diameters
There are six distinguished longitudinal fetal skull diameters:
- Suboccipito-bregmatic: from the center of anterior fontanelle (bregma) to the occipital protuberance, measuring 9.5 cm. This is the presenting diameter in vertex presentation.
- Suboccipito-frontal: from the anterior part of bregma to the occipital protuberance, measuring 10 cm
- Occipito-frontal: from the root of the nose to the most prominent part of the occiput, measuring 11.5cm
- Submento-bregmatic: from the center of the bregma to the angle of the mandible, measuring 9.5 cm. This is the presenting diameter in face presentation where the neck is hyperextended.
- Submento-vertical: from the midpoint between fontanelles and the angle of the mandible, measuring 11.5cm
- Occipito-mental: from the midpoint between fontanelles and the tip of the chin, measuring 13.5 cm. It is the presenting diameter in brow presentation.
Cardinal Movements of Normal Labor
- Neck flexion
- Internal rotation
- Extension (delivers head)
- External rotation (Restitution)
- Expulsion (delivery of anterior and posterior shoulders)
Some of the key movements are not possible in the face or brow presentations.
Based on the information provided above, it is obvious that labor will be arrested in brow presentation unless it spontaneously changes to face or vertex, as the occipito-mental diameter of the fetal head is significantly wider than the smallest diameter of the female pelvis. Face presentation can, however, be delivered vaginally, and further mechanisms of face delivery will be explained in later sections.
Indications
As mentioned previously, spontaneous vaginal delivery can be successful in face presentation. However, the main indication for vaginal delivery in such circumstances would be a maternal choice. It is crucial to have a thorough conversation with a mother, explaining the risks and benefits of vaginal delivery with face presentation and a cesarean section. Informed consent and creating a rapport with the mother is an essential aspect of safe and successful labor.
Contraindications
Vaginal delivery of face presentation is contraindicated if the mentum is lying posteriorly or is in a transverse position. In such a scenario, the fetal brow is pressing against the maternal symphysis pubis, and the short fetal neck, which is already maximally extended, cannot span the surface of the maternal sacrum. In this position, the diameter of the head is larger than the maternal pelvis, and it cannot descend through the birth canal. Therefore the cesarean section is recommended as the safest mode of delivery for mentum posterior face presentations.
Attempts to manually convert face presentation to vertex, manual or forceps rotation of the persistent posterior chin to anterior are contraindicated as they can be dangerous.
Persistent brow presentation itself is a contraindication for vaginal delivery unless the fetus is significantly small or the maternal pelvis is large.
Continuous electronic fetal heart rate monitoring is recommended for face and brow presentations, as heart rate abnormalities are common in these scenarios. One study found that only 14% of the cases with face presentation had no abnormal traces on the cardiotocograph. [8] It is advised to use external transducer devices to prevent damage to the eyes. When internal monitoring is inevitable, it is suggested to place monitoring devices on bony parts carefully.
People who are usually involved in the delivery of face/ brow presentation are:
- Experienced midwife, preferably looking after laboring woman 1:1
- Senior obstetrician
- Neonatal team - in case of need for resuscitation
- Anesthetic team - to provide necessary pain control (e.g., epidural)
- Theatre team - in case of failure to progress and an emergency cesarean section will be required.
Preparation
No specific preparation is required for face or brow presentation. However, it is essential to discuss the labor options with the mother and birthing partner and inform members of the neonatal, anesthetic, and theatre co-ordinating teams.
Technique or Treatment
Mechanism of Labor in Face Presentation
During contractions, the pressure exerted by the fundus of the uterus on the fetus and pressure of amniotic fluid initiate descent. During this descent, the fetal neck extends instead of flexing. The internal rotation determines the outcome of delivery, if the fetal chin rotates posteriorly, vaginal delivery would not be possible, and cesarean section is permitted. The approach towards mentum-posterior delivery should be individualized, as the cases are rare. Expectant management is acceptable in multiparous women with small fetuses, as a spontaneous mentum-anterior rotation can occur. However, there should be a low threshold for cesarean section in primigravida women or women with large fetuses.
When the fetal chin is rotated towards maternal symphysis pubis as described as mentum-anterior; in these cases further descend through the vaginal canal continues with approximately 73% cases deliver spontaneously. [9] Fetal mentum presses on the maternal symphysis pubis, and the head is delivered by flexion. The occiput is pointing towards the maternal back, and external rotation happens. Shoulders are delivered in the same manner as in vertex delivery.
Mechanism of Labor in Brow Presentation
As this presentation is considered unstable, it is usually converted into a face or an occiput presentation. Due to the cephalic diameter being wider than the maternal pelvis, the fetal head cannot engage; thus, brow delivery cannot take place. Unless the fetus is small or the pelvis is very wide, the prognosis for vaginal delivery is poor. With persistent brow presentation, a cesarean section is required for safe delivery.
Complications
As the cesarean section is becoming a more accessible mode of delivery in malpresentations, the incidence of maternal and fetal morbidity and mortality during face presentation has dropped significantly. [10]
However, there are still some complications associated with the nature of labor in face presentation. Due to the fetal head position, it is more challenging for the head to engage in the birth canal and descend, resulting in prolonged labor.
Prolonged labor itself can provoke foetal distress and arrhythmias. If the labor arrests or signs of fetal distress appear on CTG, the recommended next step in management is an emergency cesarean section, which in itself carries a myriad of operative and post-operative complications.
Finally, due to the nature of the fetal position and prolonged duration of labor in face presentation, neonates develop significant edema of the skull and face. Swelling of the fetal airway may also be present, resulting in respiratory distress after birth and possible intubation.
Clinical Significance
During vertex presentation, the fetal head flexes, bringing the chin to the chest, forming the smallest possible fetal head diameter, measuring approximately 9.5cm. With face and brow presentation, the neck hyperextends, resulting in greater cephalic diameters. As a result, the fetal head will engage later, and labor will progress more slowly. Failure to progress in labor is also more common in both presentations compared to vertex presentation.
Furthermore, when the fetal chin is in a posterior position, this prevents further flexion of the fetal neck, as browns are pressing on the symphysis pubis. As a result, descend through the birth canal is impossible. Such presentation is considered undeliverable vaginally and requires an emergency cesarean section.
Manual attempts to change face presentation to vertex, manual or forceps rotation to mentum anterior are considered dangerous and are discouraged.
Enhancing Healthcare Team Outcomes
A multidisciplinary team of healthcare experts supports the woman and her child during labor and the perinatal period. For a face or brow presentation to be appropriately diagnosed, an experienced midwife and obstetrician must be involved in the vaginal examination and labor monitoring. As fetal anomalies, such as anencephaly or goiter, can contribute to face presentation, sonographers experienced in antenatal scanning should also be involved in the care. It is advised to inform the anesthetic and neonatal teams in advance of the possible need for emergency cesarean section and resuscitation of the neonate. [11] [12]
Gardberg M,Leonova Y,Laakkonen E, Malpresentations--impact on mode of delivery. Acta obstetricia et gynecologica Scandinavica. 2011 May; [PubMed PMID: 21501123]
Tapisiz OL,Aytan H,Altinbas SK,Arman F,Tuncay G,Besli M,Mollamahmutoglu L,Danışman N, Face presentation at term: a forgotten issue. The journal of obstetrics and gynaecology research. 2014 Jun; [PubMed PMID: 24888918]
Zayed F,Amarin Z,Obeidat B,Obeidat N,Alchalabi H,Lataifeh I, Face and brow presentation in northern Jordan, over a decade of experience. Archives of gynecology and obstetrics. 2008 Nov; [PubMed PMID: 18283473]
Bashiri A,Burstein E,Bar-David J,Levy A,Mazor M, Face and brow presentation: independent risk factors. The journal of maternal-fetal [PubMed PMID: 18570114]
Shaffer BL,Cheng YW,Vargas JE,Laros RK Jr,Caughey AB, Face presentation: predictors and delivery route. American journal of obstetrics and gynecology. 2006 May; [PubMed PMID: 16647888]
Bellussi F,Ghi T,Youssef A,Salsi G,Giorgetta F,Parma D,Simonazzi G,Pilu G, The use of intrapartum ultrasound to diagnose malpositions and cephalic malpresentations. American journal of obstetrics and gynecology. 2017 Dec; [PubMed PMID: 28743440]
Ghi T,Eggebø T,Lees C,Kalache K,Rozenberg P,Youssef A,Salomon LJ,Tutschek B, ISUOG Practice Guidelines: intrapartum ultrasound. Ultrasound in obstetrics [PubMed PMID: 29974596]
Benedetti TJ,Lowensohn RI,Truscott AM, Face presentation at term. Obstetrics and gynecology. 1980 Feb; [PubMed PMID: 7352081]
Ducarme G,Ceccaldi PF,Chesnoy V,Robinet G,Gabriel R, [Face presentation: retrospective study of 32 cases at term]. Gynecologie, obstetrique [PubMed PMID: 16630740]
Cruikshank DP,Cruikshank JE, Face and brow presentation: a review. Clinical obstetrics and gynecology. 1981 Jun; [PubMed PMID: 7307363]
Domingues AP,Belo A,Moura P,Vieira DN, Medico-legal litigation in Obstetrics: a characterization analysis of a decade in Portugal. Revista brasileira de ginecologia e obstetricia : revista da Federacao Brasileira das Sociedades de Ginecologia e Obstetricia. 2015 May; [PubMed PMID: 26107576]
. Intrapartum care for healthy women and babies. 2022 Dec 14:(): [PubMed PMID: 32212591]
Use the mouse wheel to zoom in and out, click and drag to pan the image

- 2022 New Pearls of Exxcellence Articles
Management of Brow, Face, and Compound Malpresentations
Author: Meera Kesavan, MD
Mentor: Lisa Keder MD Editor: Daniel JS Martingano DO MBA PhD
Registered users can also download a PDF or listen to a podcast of this Pearl. Log in now , or create a free account to access bonus Pearls features.
Fetal malpresentation, including brow, face, or compound presentations, complicates around 3-4% of all term births. Because these abnormal fetal presentations still are cephalic, many such cases result in vaginal deliveries, yet there are increased risks for adverse outcomes, including cesarean delivery resultant surgical complications, persistent malpresentation precluding vaginal delivery, and abnormal labor resulting in arrest of dilation or descent.
These fetal malpresentation are differentiated in the following ways:
- In face presentations, the presenting part is the mentum, which is further divided based on its position, including mentum posterior, mentum transverse or mentum anterior positions. This typically occurs because of hyperextension of the neck and the occiput touching the fetal back. Mentum anterior malpresentations can potentially achieve vaginal deliveries, whereas mentum posterior malpresentations cannot.
- In brow presentations, there is less extension of the fetal neck as in face presentations making the leading fetal part being the area between the anterior fontanelle and the orbital ridges. These presentations are uncommon and are managed similarly to face presentations. Brow presentation can be further described based on the position of the anterior fontanelle as frontal anterior, posterior, or transverse.
- Compound presentation is defined as the leading fetal part, including a fetal extremity, alongside a cephalic or breech presentation. Management of compound presentations is expected (and often incidentally noted following delivery) because the extremity will often either retract as the head descends or will feasibly allow for delivery in its current position, with manipulation attempts to reduce the compound presentation usually avoided.
Risk factors for brow and face presentations include fetal CNS malformations, congenital or chromosomal anomalies, advanced maternal age, low birthweight, abnormal maternal pelvic anatomy (e.g. contracted pelvis, cephalopelvic disporotion, platypelloid pelvis, etc.) and nulliparity. non-Hispanic White women have the highest risk for malpresentation, whereas non-Hispanic Black women have the lowest risk.
Diagnosis usually is made during the second stage of labor while performing routine vaingla examinations and involves palpation of the abnormal leading fetal part (forehead, orbital ridge, orbits, nose, etc.) Obstetric ultrasound can additionally provide complimentary information to support these diagnoses and distinguish from other fetal malpresentations or malpositions. In face presentation, the mentum (chin) and mouth are palpable.
Management considerations for face, brow, and compounds presentations are unique with compound presentations having higher rates of vaginal delivery and lower complications as compared to either brow or face presentations.
- For brow presentations, approximately 30-40% of brow presentations will convert to a face presentation, and about 20% will convert to a vertex presentation. Anterior positions have the possibility of vaginal deliveries and can be managed by usual labor management principles, whereas mentum posterior positions are indications for cesarean delivery.
- For face presentations, the likelihood of vaginal delivery depends on the orientation of the mentum, with mentum anterior being most suitable for vaginal delivery. If the fetus is mentum posterior, flexion of the neck is precluded and results in the inability of fetal descent.
- For compound presentations, management is expectant and manipulation of the leading extremities should be avoided. Most cases of compound presentation result in vaginal deliveries. For term deliveries, compound presentations with parts other than the hand are unlikely to result in safe vaginal delivery.
Labor management for brow and face presentation overall involves continuous fetal heart rate monitoring and repeat clinical assessments, given the increased potential of fetal complications as noted. Caution should be used with internal monitoring devices, which can cause ophthalmic injury or trauma to the presenting fetal parts, with the use of fetal scalp electrodes discouraged and intrauterine pressure catheters acceptable with appropriate clinical judgment and feasibility.
Midforceps, breech extraction, and manual manipulation are not recommended and increase the risk of maternal and neonatal morbidity.
Neonatal outcomes for both face and brow presentations include facial edema, bruising, and soft tissue trauma. Complications of compound presentation specifically include umbilical cord prolapse and injury to the presenting limb. With appropriate management, neonatal and maternal morbidity for face, brow, and compound presentations are low.
Further Reading:
Bar-El L, Eliner Y, Grunebaum A, Lenchner E, et al. Race and ethnicity are among the predisposing factors for fetal malpresentation at term. Am J Obstet Gynecol MFM. 2021 Sep;3(5):100405. doi: 10.1016/j.ajogmf.2021.100405. Epub 2021 Jun 4. PMID: 34091061.
Bellussi F, Ghi T, Youssef A, et al. The use of intrapartum ultrasound to diagnose malpositions and cephalic malpresentations. Am J Obstet Gynecol. 2017 Dec;217(6):633-641. doi: 10.1016/j.ajog.2017.07.025. Epub 2017 Jul 22. PMID: 28743440 .
Pilliod RA, Caughey AB. Fetal Malpresentation and Malposition: Diagnosis and Management. Obstet Gynecol Clin North Am. 2017 Dec;44(4):631-643. doi: 10.1016/j.ogc.2017.08.003. PMID: 29078945 .
Zayed F, Amarin Z, Obeidat B, et al. Face and brow presentation in northern Jordan, over a decade of experience. Arch Gynecol Obstet. 2008 Nov;278(5):427-30. doi: 10.1007/s00404-008-0600-0. Epub 2008 Feb 19. PMID: 18283473 .
Initial Approval: August 2013; Revised: 11/2016; Revised July 2018; Reaffirmed January 2020; Revised September 2021. Revised July 2023.
This site uses cookies.

This feature is only available for registered users.
Log in here:, not a registered user.
Becoming a registered user gives you access to special features like PDF downloads and podcast episodes of each SASGOG Pearl of Exxcellence.
Create a Free Account
Are you sure you want to remove this Pearl from your favorites list?
GFMER Geneva Foundation for Medical Education and Research
- Annual reports
- GFMER members
- Country coordinators
- Obstetric fistula
- Cervical cancer
- Emergency and surgical care
- Picture of the week
- Social media
- Free medical journals
Obstetrics Simplified - Diaa M. EI-Mowafi
Brow Presentation
It is a cephalic presentation in which the head is midway between flexion and extension.
About 1:1000 labour.
As face presentation.
- It is difficult.
- The occiput and sinciput may be felt at the same level.
- Ultrasonography and X-ray may be helpful.
- frontal bones,
- supra-orbital ridges, and
- root of the nose but not the chin.
Mechanism of Labour
- The engagement diameter is the mento-vertical 13.5 cm which is longer than any diameter of the inlet so there is no mechanism of labour and labour is obstructed.
- may occur during conversion of vertex into face presentation. So if brow is flexed to become vertex or extended to become face it may be delivered.
- Exclude contracted pelvis, if present do caesarean section.
- The case is considered as transient brow, observed carefully and given a chance for spontaneous conversion into either face or vertex.
- The rest of management as other malpresentation.
- Caesarean section is done if the foetus is living.
- Craniotomy if the foetus is dead.
- Dystocia : Guidelines, reviews
Brow Presentation
- First Online: 02 August 2023
Cite this chapter

- Syeda Batool Mazhar 2 &
- Zahra Ahmed Muslim 2
474 Accesses
Brow presentation is the rarest of all malpresentations. Anencephaly, neck masses in fetus, polyhydramnios, multiple loops of cord around neck are the fetal factors leading to brow presentation. Contracted pelvis, preterm labour, platypelloid pelvis are some of the contributory maternal factors for brow presentation. Diagnosis is usually made during second stage of labour during prevaginal examination when anterior frontanelle and face are palpated. Cesarean section is performed in brow presentation as it is unusual to get conversion in average sized fetus once membranes have ruptured.
This is a preview of subscription content, log in via an institution to check access.
Access this chapter
- Available as PDF
- Read on any device
- Instant download
- Own it forever
- Available as EPUB and PDF
- Durable hardcover edition
- Dispatched in 3 to 5 business days
- Free shipping worldwide - see info
Tax calculation will be finalised at checkout
Purchases are for personal use only
Institutional subscriptions
Arulkumaran S, Robson M, editors. Munro Kerr operative obstetrics. 13th ed. Elsevier, Amsterdam; 2019. p. 89–93.
Google Scholar
Malvasi A, Barbera A, Di Vagno G, Gimovsky A, Berghella V, Ghi T, Di Renzo GC, Tinelli A. Asynclitism: a literature review of an often forgotten clinical condition. J Matern Fetal Neonatal Med. 2015;28(16):1890–4. https://doi.org/10.3109/14767058.2014.972925 . Epub 2014 Oct 29.PMID: 25283847.
Article PubMed Google Scholar
Bellussi F, Ghi T, Youssef A, Salsi G, Giorgetta F, Parma D, Simonazzi G, Gianluigi P. The use of intrapartum ultrasound to diagnose malpositions and cephalic malpresentations. Am J Obstet Gynecol. 2017;217(6):633–41.
Lanni SM, Gherman R, Gonik B. Malpresentations. Amsterdam: Elsevier; 2017.
Book Google Scholar
Bashiri A, Burstein E, Bar-David J, et al. Face and brow presentation: independent risk factors. J Matern Fetal Neonatal Med. 2008;21(6):357–60.
Hawkins JL, Koffel BL. Chapter 35. In: Chestnut’s obstetric anesthesia: principles and practice: abnormal presentation & multiple gestation. 6th ed; 2020. p. 830.
Meltzer RM, Sactleben MR, Friedman EA. Brow presentation. Obstet Gynecol Surv. 1968;23(6):255–63.
Article Google Scholar
Borell U, Fernstrom I. The mechanism of labour in face and brow presentation: a radiological study. Acta Obstet Gynecol Scand. 1960;39:626–44.
Article CAS PubMed Google Scholar
Levy DL. Persistent brow presentation: a new approach to management. South Med J. 1976;69(2):191–2.
Download references
Author information
Authors and affiliations.
MCH Centre, PIMS, Islamabad, Pakistan
Syeda Batool Mazhar & Zahra Ahmed Muslim
You can also search for this author in PubMed Google Scholar
Editor information
Editors and affiliations.
Department of Obstetrics and Gynecology, Sarojini Naidu Medical College, Agra, Uttar Pradesh, India
Ruchika Garg
Rights and permissions
Reprints and permissions
Copyright information
© 2023 The Author(s), under exclusive license to Springer Nature Singapore Pte Ltd.
About this chapter
Mazhar, S.B., Muslim, Z.A. (2023). Brow Presentation. In: Garg, R. (eds) Labour and Delivery. Springer, Singapore. https://doi.org/10.1007/978-981-19-6145-8_8
Download citation
DOI : https://doi.org/10.1007/978-981-19-6145-8_8
Published : 02 August 2023
Publisher Name : Springer, Singapore
Print ISBN : 978-981-19-6144-1
Online ISBN : 978-981-19-6145-8
eBook Packages : Medicine Medicine (R0)
Share this chapter
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Publish with us
Policies and ethics
- Find a journal
- Track your research
Persistent brow presentation: a new approach to management
- PMID: 1251243
- DOI: 10.1097/00007611-197602000-00019
When the fetal vertex is extended on the spinal column and the brow becomes the presenting part, it is termed "brow presentation." Persistent brow presentation occurs when there is no spontaneous conversion after the onset of active labor. Since there is a risk in the vaginal delivery of such fetuses, it should not be attempted where there is known maternal disease or evidence of acute or chronic intrauterine fetal distress. During labor, cesarean section is indicated if there is cephalopelvic disproportion, if the fetal head is not in the frontoanterior position, if there is abnormal labor, or if there is evidence of fetal distress. Continuous lumbar epidural anesthesia should be given, and only manual conversion is used. The fetus is monitored continuously.
- Anesthesia, Epidural
- Anesthesia, Obstetrical
- Delivery, Obstetric / methods
- Fetal Distress / diagnosis
- Fetus / physiology
- Labor Presentation*
- GP practice services
- Health advice
- Health research
- Medical professionals
Health topics
Advice and clinical information on a wide variety of healthcare topics.
All health topics
Latest features
Allergies, blood & immune system
Bones, joints and muscles
Brain and nerves
Chest and lungs
Children's health
Cosmetic surgery
Digestive health
Ear, nose and throat
General health & lifestyle
Heart health and blood vessels
Kidney & urinary tract
Men's health
Mental health
Oral and dental care
Senior health
Sexual health
Signs and symptoms
Skin, nail and hair health
Travel and vaccinations
Treatment and medication
Women's health
Healthy living
Expert insight and opinion on nutrition, physical and mental health.
Exercise and physical activity
Healthy eating
Healthy relationships
Managing harmful habits
Mental wellbeing
Relaxation and sleep
Managing conditions
From ACE inhibitors for high blood pressure, to steroids for eczema, find out what options are available, how they work and the possible side effects.
Featured conditions
ADHD in children
Crohn's disease
Endometriosis
Fibromyalgia
Gastroenteritis
Irritable bowel syndrome
Polycystic ovary syndrome
Scarlet fever
Tonsillitis
Vaginal thrush
Health conditions A-Z
Medicine information
Information and fact sheets for patients and professionals. Find out side effects, medicine names, dosages and uses.
All medicines A-Z
Allergy medicines
Analgesics and pain medication
Anti-inflammatory medicines
Breathing treatment and respiratory care
Cancer treatment and drugs
Contraceptive medicines
Diabetes medicines
ENT and mouth care
Eye care medicine
Gastrointestinal treatment
Genitourinary medicine
Heart disease treatment and prevention
Hormonal imbalance treatment
Hormone deficiency treatment
Immunosuppressive drugs
Infection treatment medicine
Kidney conditions treatments
Muscle, bone and joint pain treatment
Nausea medicine and vomiting treatment
Nervous system drugs
Reproductive health
Skin conditions treatments
Substance abuse treatment
Vaccines and immunisation
Vitamin and mineral supplements
Tests & investigations
Information and guidance about tests and an easy, fast and accurate symptom checker.
About tests & investigations
Symptom checker
Blood tests
BMI calculator
Pregnancy due date calculator
General signs and symptoms
Patient health questionnaire
Generalised anxiety disorder assessment
Medical professional hub
Information and tools written by clinicians for medical professionals, and training resources provided by FourteenFish.
Content for medical professionals
FourteenFish training
- Professional articles
Evidence-based professional reference pages authored by our clinical team for the use of medical professionals.
View all professional articles A-Z
Actinic keratosis
Bronchiolitis
Molluscum contagiosum
Obesity in adults
Osmolality, osmolarity, and fluid homeostasis
Recurrent abdominal pain in children
Medical tools and resources
Clinical tools for medical professional use.
All medical tools and resources
Malpresentations and malpositions
Peer reviewed by Dr Laurence Knott Last updated by Dr Colin Tidy, MRCGP Last updated 22 Jun 2021
Meets Patient’s editorial guidelines
Medical Professionals
Professional Reference articles are designed for health professionals to use. They are written by UK doctors and based on research evidence, UK and European Guidelines. You may find one of our health articles more useful.
In this article :
Malpresentation, malposition.
Usually the fetal head engages in the occipito-anterior position (more often left occipito-anterior (LOA) rather than right) and then undergoes a short rotation to be directly occipito-anterior in the mid-cavity. Malpositions are abnormal positions of the vertex of the fetal head relative to the maternal pelvis. Malpresentations are all presentations of the fetus other than vertex.
Obstetrics - the pelvis and head

Continue reading below
Predisposing factors to malpresentation include:
Prematurity.
Multiple pregnancy.
Abnormalities of the uterus - eg, fibroids.
Partial septate uterus.
Abnormal fetus.
Placenta praevia.
Primiparity.
Breech presentation
See the separate Breech Presentations article for more detailed discussion.
Breech presentation is the most common malpresentation, with the majority discovered before labour. Breech presentation is much more common in premature labour.
Approximately one third are diagnosed during labour when the fetus can be directly palpated through the cervix.
After 37 weeks, external cephalic version can be attempted whereby an attempt is made to turn the baby manually by manipulating the pregnant mother's abdomen. This reduces the risk of non-cephalic delivery 1 .
Maternal postural techniques have also been tried but there is insufficient evidence to support these 2 .
Many women who have a breech presentation can deliver vaginally. Factors which make this less likely to be successful include 3 :
Hyperextended neck on ultrasound.
High estimated fetal weight (more than 3.8 kg).
Low estimated weight (less than tenth centile).
Footling presentation.
Evidence of antenatal fetal compromise.
Transverse lie 4
When the fetus is positioned with the head on one side of the pelvis and the buttocks in the other (transverse lie), vaginal delivery is impossible.
This requires caesarean section unless it converts or is converted late in pregnancy. The surgeon may be able to rotate the fetus through the wall of the uterus once the abdominal wall has been opened. Otherwise, a transverse uterine incision is needed to gain access to a fetal pole.
Internal podalic version is no longer attempted.
Transverse lie is associated with a risk of cord prolapse of up to 20%.
Occipito-posterior position
This is the most common malposition where the head initially engages normally but then the occiput rotates posteriorly rather than anteriorly. 5.2% of deliveries are persistent occipito-posterior 5 .
The occipito-posterior position results from a poorly flexed vertex. The anterior fontanelle (four radiating sutures) is felt anteriorly. The posterior fontanelle (three radiating sutures) may also be palpable posteriorly.
It may occur because of a flat sacrum, poorly flexed head or weak uterine contractions which may not push the head down into the pelvis with sufficient strength to produce correct rotation.
As occipito-posterior-position pregnancies often result in a long labour, close maternal and fetal monitoring are required. An epidural is often recommended and it is essential that adequate fluids be given to the mother.
The mother may get the urge to push before full dilatation but this must be discouraged. If the head comes into a face-to-pubis position then vaginal delivery is possible as long as there is a reasonable pelvic size. Otherwise, forceps or caesarean section may be required.
Occipito-transverse position
The head initially engages correctly but fails to rotate and remains in a transverse position.
Alternatives for delivery include manual rotation of fetal head using Kielland's forceps, or delivery using vacuum extraction. This is inappropriate if there is any fetal acidosis because of the risk of cerebral haemorrhage.
Therefore, there must be provision for a failure of forceps delivery to be changed immediately to a caesarean. The trial of forceps is therefore often performed in theatre. Some centres prefer to manage by caesarean section without trial of forceps.
Face presentations
Face presents for delivery if there is complete extension of the fetal head.
Face presentation occurs in 1 in 1,000 deliveries 5 .
With adequate pelvic size, and rotation of the head to the mento-anterior position, vaginal delivery should be achieved after a long labour.
Backwards rotation of the head to a mento-posterior position requires a caesarean section.
Brow positions
The fetal head stays between full extension and full flexion so that the biggest diameter (the mento-vertex) presents.
Brow presentation occurs in 0.14% of deliveries 5 .
Brow presentation is usually only diagnosed once labour is well established.
The anterior fontanelle and super orbital ridges are palpable on vaginal examination.
Unless the head flexes, a vaginal delivery is not possible, and a caesarean section is required.
Further reading and references
- Hofmeyr GJ, Kulier R, West HM ; External cephalic version for breech presentation at term. Cochrane Database Syst Rev. 2015 Apr 1;(4):CD000083. doi: 10.1002/14651858.CD000083.pub3.
- Hofmeyr GJ, Kulier R ; Cephalic version by postural management for breech presentation. Cochrane Database Syst Rev. 2012 Oct 17;10:CD000051. doi: 10.1002/14651858.CD000051.pub2.
- Management of Breech Presentation ; Royal College of Obstetricians and Gynaecologists (Mar 2017)
- Szaboova R, Sankaran S, Harding K, et al ; PLD.23 Management of transverse and unstable lie at term. Arch Dis Child Fetal Neonatal Ed. 2014 Jun;99 Suppl 1:A112-3. doi: 10.1136/archdischild-2014-306576.324.
- Gardberg M, Leonova Y, Laakkonen E ; Malpresentations - impact on mode of delivery. Acta Obstet Gynecol Scand. 2011 May;90(5):540-2. doi: 10.1111/j.1600-0412.2011.01105.x.
Article History
The information on this page is written and peer reviewed by qualified clinicians.
Next review due: 21 Jun 2026
22 jun 2021 | latest version.
Last updated by
Peer reviewed by

Feeling unwell?
Assess your symptoms online for free
IMAGES
VIDEO
COMMENTS
Persistent brow presentation itself is a contraindication for vaginal delivery unless the fetus is significantly small or the maternal pelvis is large. Equipment. Continuous electronic fetal heart rate monitoring is recommended for face and brow presentations, as heart rate abnormalities are common in these scenarios. ...
The brow may convert to a vertex presentation, to a face presentation, or remain as a persistent brow presentation. More than 50% of brow presentations will convert to vertex or face presentation and labor courses are managed accordingly when spontaneous conversion occurs. In the brow presentation, the occipitomental diameter, which is the ...
The vast majority of fetuses at term are in cephalic presentation. Approximately 5 percent of these fetuses are in a cephalic malpresentation, such as occiput posterior or transverse, face ( figure 1A-B ), or brow ( figure 2) [ 1 ]. Diagnosis and management of face and brow presentations will be reviewed here.
7.10.1 Diagnosis. 7.10.2 Management. Foetus alive. Foetus dead. Brow presentation constitutes an absolute foeto-pelvic disproportion, and vaginal delivery is impossible (except with preterm birth or extremely low birth weight). This is an obstetric emergency, because labour is obstructed and there is a risk of uterine rupture and foetal distress.
One such complication that can come at the last minute of any delivery is the presentation of the baby. Normally, babies bow down their chin well tucked into the chest during their journey through the birth canal. This position is called flexed position or vertex presentation. This is the ideal position that makes delivery easier as the baby ...
Persistent brow presentation itself is a contraindication for vaginal delivery unless the fetus is significantly small or the maternal pelvis is large. Equipment. Continuous electronic fetal heart rate monitoring is recommended for face and brow presentations, as heart rate abnormalities are common in these scenarios. ...
Five percent of fetuses present in brow, face, or compound presentations, many of which result in vaginal delivery. Patients should be counseled about increased risk for cesarean delivery due to fetal distress, labor arrest, or persistent malpresentations. Risk factors for brow and face presentations include anencephaly, hydrocephalus, fetal neck masses, cephalopelvic disproportion ...
The outlook of the persistent brow presentation for vaginal delivery is poor. Approximately two thirds of brow presentations will convert to vertex or face. 2 Fortunately, this is a rare presentation, with an incidence of only 0.05%. 5 If the presentation persists as a brow, a cesarean section should be performed.
Persistent brow: The engagement diameter is the mento-vertical 13.5 cm which is longer than any diameter of the inlet so there is no mechanism of labour and labour is obstructed. Transient brow: may occur during conversion of vertex into face presentation. So if brow is flexed to become vertex or extended to become face it may be delivered ...
Brow presentation is the rarest of all malpresentations. Anencephaly, neck masses in fetus, polyhydramnios, multiple loops of cord around neck are the fetal factors leading to brow presentation. ... Generally, majority of persistent brow presentations are associated with factors that delay the engagement of head . These include. 1. Maternal ...
Introduction. Face presentation is a rare unanticipated obstetric event characterized by a longitudinal lie and full extension of the foetal head on the neck with the occiput against the upper back [1-3].Face presentation occurs in 0.1-0.2% of deliveries [3-5] but is more common in black women and in multiparous women [].Studies have shown that 60 per cent of face presentations have one or ...
rarely occurring persistent brow presenta tion. Because of the low incidence, most studies have dealt with comparatively small numbers of cases and some have included data for face presentation as well.S' 10, II, 13, 15-19,21,22 In an attempt to examine a larger series of brow presentations for analysis, the
Brow: brow presentation represents deflexion of the fetal head but not to the same degree as the complete extension causing a face presentation, with an incidence of approximately 1 in 2000 births. In a brow presentation, the presenting diameter is mento-vertical, at approximately 13 cm, and is therefore the most unfavourable of cephalic ...
In contrast, the incidence of breech presentation and persistent occipitoposterior position seems remarkably constant. In textbooks, the incidence of breech presentation is generally stated as 3-4% and that of persistent occipitoposterior position as 4-5% of all deliveries. ... It is possible that some of the brow presentations would have ...
Persistent brow presentation occurs when there is no spontaneous conversion after the onset of active labor. Since there is a risk in the vaginal delivery of such fetuse … When the fetal vertex is extended on the spinal column and the brow becomes the presenting part, it is termed "brow presentation."
Brow positions. The fetal head stays between full extension and full flexion so that the biggest diameter (the mento-vertex) presents. Brow presentation occurs in 0.14% of deliveries 5. Brow presentation is usually only diagnosed once labour is well established. The anterior fontanelle and super orbital ridges are palpable on vaginal examination.
Background. Persistent occiput posterior (OP) position is associated with 18% of intrapartum caesarean sections and a high risk of assisted vaginal delivery [1-3].Caesarean section is now a major contributing factor to maternal mortality and morbidity following childbirth in developed countries [4,5].Obstetric intervention by forceps and ventouse delivery is associated with complications to ...
Persistent brow presentation occurs when there is no spontaneous conversion after the onset of active labor. Since there is a risk in the vaginal delivery of such fetuses, it should not be attempted where there is known maternal disease or evidence of acute or chronic intrauterine fetal distress. During labor, cesarean section is indicated if ...
Europe PMC is an archive of life sciences journal literature. Persistent brow presentation: a new approach to management.
Semantic Scholar extracted view of "Management of persistent brow presentation." by Moore Ej et al.
Full text. Full text is available as a scanned copy of the original print version. Get a printable copy (PDF file) of the complete article (305K), or click on a page image below to browse page by page.
The new Teams app now powers Teams Rooms on Windows devices. The new Teams app delivers up to two times faster performance while using 50 percent less memory. This means that Teams Rooms devices can utilize available resources to optimize the room experience and to render intelligent audio and video more reliably.
Brow presentation; spontaneous rectification to a vertex in the pelvis. J Obstet Gynaecol Br Emp. 1957 Dec; 64 (6):909-910. ... TANCER ML, ROSANELLI P. Face and persistent brow presentations. Obstet Gynecol. 1957 Dec; 10 (6):632-635. [Google Scholar] WHITE TG. Deflexion attitudes of the foetus in utero with special reference to the ...